Version 1.0 — Published April 2026
Quick Answer
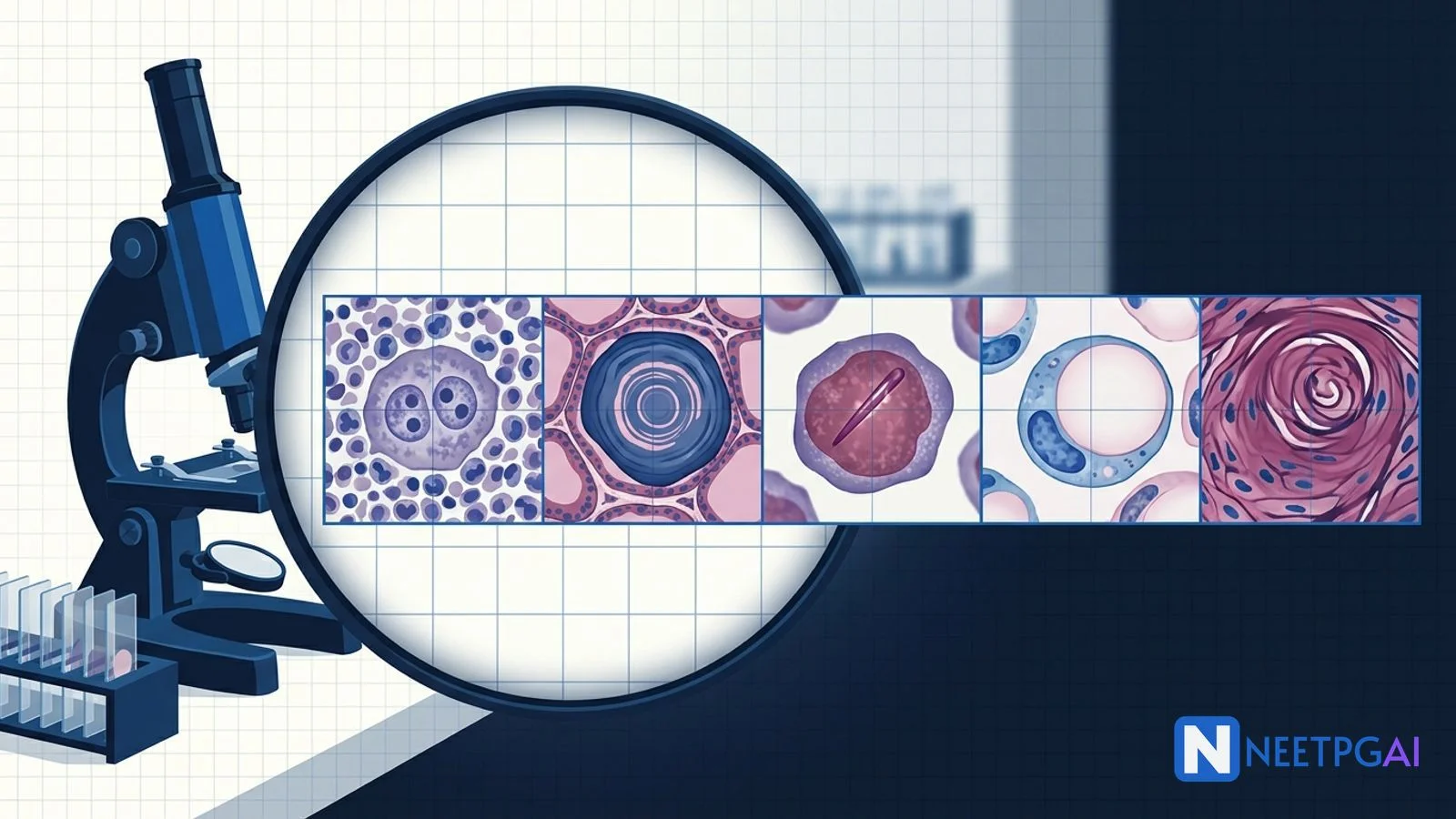
Histopathology image MCQs contribute 4-6 questions per NEET PG paper across pathology, oncology, and the surgical specialties. Five histologic patterns recur reliably: Reed-Sternberg cells (Hodgkin lymphoma), psammoma bodies (papillary thyroid, serous ovarian, meningioma, papillary renal), Auer rods (AML — bundled = M3 APL), signet ring cells (gastric and lobular breast carcinoma), and keratin pearls (well-differentiated squamous cell carcinoma).
The pattern-to-diagnosis mapping is the highest-leverage histopathology revision an exam-week student can do — each pattern produces 1-3 NEET PG questions across recent papers.
Why histopathology image MCQs are high-yield
NEET PG pathology contributes 12-15 questions per paper, of which 30-40 percent are image-based. Tumour histopathology dominates the image set because the patterns are visually distinctive and the diagnoses are clinically anchored. Unlike text questions, histology images reward instant pattern recognition: a 2-second glance gives the answer if the pattern is in your trained library. The five MCQs below cover almost every recent NEET PG histopathology question (2019-2024 papers).
For each, we walk through the image description, the four answer options, the correct answer with reasoning, and a teaching pearl. Pair this with daily 10-image histology drilling for 2 weeks and your accuracy will climb from 40 to 85 percent.
MCQ 1: 22-year-old man with painless cervical lymphadenopathy
Image description: [High-power H&E section of a lymph node showing diffuse effacement of architecture by a mixed inflammatory background of small lymphocytes, eosinophils, and plasma cells. Scattered through the field are large cells (about 30-50 micrometres) with bi-lobed or multi-lobed nuclei, prominent inclusion-like eosinophilic nucleoli surrounded by a clear halo, giving an "owl-eye" appearance. Some sections show fibrous bands separating nodules.]
Clinical vignette: A 22-year-old engineering student presents with 2 months of painless right cervical lymph node enlargement (3.5 cm), occasional drenching night sweats, 5 kg weight loss, and intermittent low-grade fever. CECT chest shows mediastinal lymphadenopathy. Excision biopsy is performed.
Options:
- (a) Reactive lymphoid hyperplasia
- (b) Diffuse large B-cell lymphoma
- (c) Classical Hodgkin lymphoma — nodular sclerosis subtype
- (d) Tuberculous lymphadenitis
Correct answer: (c) Classical Hodgkin lymphoma — nodular sclerosis subtype
Reasoning: The combination of a young adult, painless cervical-mediastinal lymphadenopathy, B-symptoms, and biopsy showing Reed-Sternberg cells (bi-nucleate, owl-eye nucleoli) on a polymorphous reactive background of lymphocytes, eosinophils, plasma cells, and histiocytes is diagnostic of classical Hodgkin lymphoma. Fibrous bands separating cellular nodules indicate the nodular sclerosis subtype — most common cHL subtype (60-70 percent), peak in adolescents and young adults, female predominance, mediastinal involvement common.
DLBCL would show a monomorphic sheet of large transformed B cells without the polymorphous background or RS cells. Reactive hyperplasia retains follicular architecture with germinal centres. Tuberculous lymphadenitis shows caseating granulomas with epithelioid histiocytes and Langhans giant cells, not RS cells.
Teaching pearl: Hodgkin lymphoma classification at NEET PG depth:
| Subtype | Frequency | Cellular pattern | RS variant |
|---|
| Nodular sclerosis (NS) | 60-70% | Fibrous bands + cellular nodules | Lacunar |
| Mixed cellularity (MC) | 20-25% | RS cells in mixed inflammatory background | Classic RS |
| Lymphocyte-rich (LR) | 5% | RS cells in lymphocyte-rich background | Classic RS |
| Lymphocyte-depleted (LD) | <5% | Few lymphocytes, many pleomorphic RS cells | Pleomorphic, mummified |
| Nodular lymphocyte-predominant (NLPHL) | Separate entity | Nodular B-cell-rich background | LP / popcorn cell (CD20+, CD30-, CD15-) |
Immunophenotype of classic RS cell: CD30+, CD15+, CD20-/weak, CD45-, PAX5+/weak, EBV in 40 percent of mixed cellularity.
Treatment principles: ABVD (adriamycin, bleomycin, vinblastine, dacarbazine) for early-stage; ABVD ± radiotherapy or BEACOPP for advanced; brentuximab vedotin (anti-CD30 ADC) and PD-1 inhibitors (nivolumab, pembrolizumab) for relapsed-refractory.
MCQ 2: 45-year-old woman with thyroid nodule and cervical lymphadenopathy
Image description: [Medium-power H&E section of a thyroid mass showing complex branching papillary structures lined by cuboidal cells with overlapping, ground-glass (Orphan-Annie-eye) nuclei, longitudinal nuclear grooves, and intranuclear pseudoinclusions. Within the papillary cores and the stroma are scattered concentric lamellated round calcified bodies (about 50-100 micrometres in diameter) resembling onion rings or sand grains.]
Clinical vignette: A 45-year-old woman presents with a 2.5 cm right thyroid nodule found on a routine USG done for vague neck discomfort. USG showed a hypoechoic solid nodule with microcalcifications, irregular margins, taller-than-wide shape, and a single 8-mm right cervical lymph node. FNAC is suggestive; right lobectomy with isthmusectomy is performed.
Options:
- (a) Follicular adenoma
- (b) Hurthle cell carcinoma
- (c) Papillary thyroid carcinoma
- (d) Medullary thyroid carcinoma
Correct answer: (c) Papillary thyroid carcinoma
Reasoning: Three diagnostic features here — (1) papillary architecture, (2) characteristic nuclear changes (ground-glass Orphan-Annie nuclei, longitudinal grooves, intranuclear pseudoinclusions), and (3) psammoma bodies. PTC is diagnosed on nuclear features alone (the encapsulated follicular variant lacks papillae but has the same nuclei). Psammoma bodies are present in about 50 percent of PTCs.
Follicular adenoma shows uniform follicles surrounded by a complete fibrous capsule; no papillae, no psammoma bodies. Hurthle cell carcinoma shows oncocytic (mitochondria-rich) cells with vascular and capsular invasion. Medullary thyroid carcinoma is a C-cell-derived tumour with sheets of polygonal cells in an amyloid stroma; calcitonin-positive on IHC; no PTC nuclear features.
Teaching pearl: The classic four locations of psammoma bodies — memorise this list for NEET PG:
| Location | Tumour |
|---|
| Thyroid | Papillary thyroid carcinoma |
| Ovary | Serous papillary cystadenocarcinoma |
| Brain | Meningioma (especially psammomatous variant) |
| Kidney | Papillary renal cell carcinoma |
Other less common: prolactinoma, mesothelioma, endometrial serous carcinoma. The mechanism is dystrophic calcification on apoptotic tumour debris within papillary structures — they need a papillary backbone to form.
PTC is the most common thyroid malignancy (75-85 percent of thyroid cancers). Risk factors include radiation exposure (especially childhood), Hashimoto thyroiditis (small association), and BRAF V600E mutation. Spreads via lymphatics (cervical lymph nodes) early but has excellent prognosis (10-year survival >95 percent for low-risk disease). Treatment: total or hemi-thyroidectomy ± radioiodine (RAI) ablation ± TSH suppression.
MCQ 3: 28-year-old woman with sudden-onset bleeding and abnormal blood counts
Image description: [Wright-Giemsa-stained bone marrow aspirate smear at 1000x oil immersion. Numerous large blast-like cells with abundant azurophilic granular cytoplasm dominate the field. The nuclei are large, lobulated or bilobed (kidney-shaped or "butterfly"-shaped) with delicate chromatin and indistinct nucleoli. Many of these cells contain bundles of needle-shaped, rod-like cytoplasmic inclusions resembling stacks of pencils — multiple per cell. The background shows decreased erythroid and megakaryocyte precursors.]
Clinical vignette: A 28-year-old woman presents to the emergency with 1 week of fatigue, low-grade fever, gum bleeding, and a single episode of haematuria today. CBC: Hb 7.2 g/dL, WBC 28,000 (with 65 percent blasts on smear), platelets 22,000. PT 19 s (control 13), aPTT 38 s, fibrinogen 110 mg/dL, D-dimer 8.4 mcg/mL.
Options:
- (a) Acute lymphoblastic leukemia
- (b) Acute promyelocytic leukemia (AML M3)
- (c) Chronic myeloid leukemia in blast crisis
- (d) Reactive lymphocytosis
Correct answer: (b) Acute promyelocytic leukemia (AML M3)
Reasoning: Bundles of Auer rods (faggot cells) plus the distinctive bilobed/butterfly-shaped nucleus and abundant azurophilic granular cytoplasm are pathognomonic of acute promyelocytic leukemia. The clinical picture — sudden bleeding, low fibrinogen, raised PT and D-dimer — is the classic DIC of APL.
ALL shows blasts with scant, agranular blue cytoplasm and a high nuclear-cytoplasmic ratio; no Auer rods (Auer rods rule out lymphoid lineage). CML blast crisis can be myeloid or lymphoid but rarely shows faggot cells. Reactive lymphocytosis would not show blasts at this level or DIC.
Teaching pearl: APL is an oncological emergency — high early mortality from intracranial and pulmonary haemorrhage if untreated. Management starts before molecular confirmation:
- Suspect APL in any AML with bleeding, faggot cells, or DIC
- Start ATRA (all-trans retinoic acid, 45 mg/m²/day) immediately on suspicion
- Add arsenic trioxide (ATO) for low-intermediate risk APL — ATRA + ATO is now standard of care, chemotherapy-free for many patients, >90 percent cure rate
- Aggressive blood-product support — platelets to keep ≥30-50,000, fibrinogen ≥150 mg/dL with cryoprecipitate, fresh frozen plasma for prolonged PT
- Watch for differentiation syndrome (formerly retinoic acid syndrome) — fever, weight gain, dyspnea, pulmonary infiltrates, pleural/pericardial effusions, hypotension; treat with dexamethasone 10 mg IV BD
Genetic hallmark: t(15;17)(q24;q21) — PML-RARA fusion. Confirmatory test: FISH or RT-PCR for PML-RARA. Variant translocations (t(11;17) PLZF-RARA) are ATRA-resistant.
Auer rods in non-APL AML: single rods in M1 (AML without maturation), M2 (AML with maturation), M4 (acute myelomonocytic leukemia), and M5 (acute monocytic leukemia). Multiple bundled rods (faggot cells) = M3 (APL).
MCQ 4: 55-year-old man with weight loss, early satiety, and dyspepsia
Image description: [Medium-power H&E section of a gastric biopsy showing extensive infiltration of the gastric submucosa by single discohesive tumour cells. Each cell has abundant clear cytoplasm filled with mucin, with the nucleus pushed to the cell periphery and flattened against the cell membrane, creating a half-moon shape — resembling a signet ring or a class ring. The cells lie singly or in small clusters in a desmoplastic stroma; no glandular structures are seen.]
Clinical vignette: A 55-year-old labourer presents with 3 months of vague epigastric pain, early satiety, weight loss of 8 kg, and one episode of melena. Endoscopy shows a thickened, rigid, non-distensible stomach with absent rugae — "leather-bottle" appearance. Multiple biopsies are taken from the body and antrum.
Options:
- (a) Gastric MALT lymphoma
- (b) Gastrointestinal stromal tumour (GIST)
- (c) Diffuse-type (signet ring cell) gastric adenocarcinoma — Lauren classification
- (d) Pancreatic adenocarcinoma metastatic to stomach
Correct answer: (c) Diffuse-type (signet ring cell) gastric adenocarcinoma
Reasoning: Signet ring cells infiltrating the gastric wall in a diffuse, single-file or single-cell pattern with desmoplasia — the histologic signature of the Lauren diffuse-type gastric adenocarcinoma. The "leather bottle stomach" (linitis plastica) on endoscopy or barium meal corresponds clinically.
MALT lymphoma shows lymphoepithelial lesions with monotonous small B cells; CD20 positive. GIST is mesenchymal — spindle or epithelioid cells, CD117 (KIT) positive, DOG1 positive, no signet ring morphology. Pancreatic metastasis to stomach is uncommon and would have ductal architecture with mucin secretion patterns, not signet ring cells.
Teaching pearl: Lauren classification of gastric adenocarcinoma:
| Type | Histology | Demographics | Risk factors |
|---|
| Intestinal | Glandular, cohesive | Older, men > women | H. pylori, chronic atrophic gastritis, intestinal metaplasia |
| Diffuse | Signet ring, single cells, linitis plastica | Younger, women = men | E-cadherin loss (CDH1 mutation in hereditary diffuse gastric cancer), blood group A |
Hereditary diffuse gastric cancer (HDGC): CDH1 germline mutation → diffuse gastric cancer plus lobular breast cancer (also signet ring). Prophylactic total gastrectomy considered.
Other signet ring cell tumours:
- Invasive lobular breast carcinoma — single-file Indian-file pattern, E-cadherin loss (same molecular background as HDGC)
- Colorectal mucinous adenocarcinoma with signet ring component (poor prognosis)
- Pulmonary mucinous adenocarcinoma
- Krukenberg tumour — bilateral ovarian metastases from primary gastric or breast signet ring carcinoma; histology shows signet ring cells in ovarian stroma. Always look for a primary in the GI tract or breast.
MCQ 5: 62-year-old smoker with persistent oral ulcer
Image description: [Medium-power H&E section of an oral cavity biopsy showing irregular nests and cords of polygonal cells with abundant pink eosinophilic cytoplasm, distinct cell borders with visible intercellular bridges, infiltrating into the underlying connective tissue stroma. Within the nests, concentric whorled aggregates of cells with central laminated bright pink keratin material are scattered throughout — measuring 50-200 micrometres each. Mitotic figures are present but moderate.]
Clinical vignette: A 62-year-old man, lifelong bidi smoker and tobacco-chewer, presents with a non-healing ulcer on the right lateral border of the tongue, persisting for 3 months despite local antiseptics. The ulcer is 2.5 cm, indurated, with raised everted edges. He has palpable level Ib and II right cervical lymph nodes.
Options:
- (a) Aphthous ulcer
- (b) Tuberculous ulcer
- (c) Well-differentiated squamous cell carcinoma
- (d) Adenoid cystic carcinoma
Correct answer: (c) Well-differentiated squamous cell carcinoma
Reasoning: Keratin pearls (concentric squamous whorls with central keratinisation) plus intercellular bridges at high power — the histologic hallmarks of well-differentiated squamous cell carcinoma. The clinical setting (chronic non-healing oral ulcer, indurated, in a tobacco user with cervical lymph nodes) confirms the diagnosis.
Aphthous ulcer is a small painful ulcer with white-yellow base and erythematous margin; histology shows non-specific inflammation, no atypical squamous nests. Tuberculous ulcer shows caseating granulomas with Langhans giant cells; rare in the oral cavity. Adenoid cystic carcinoma shows cribriform "Swiss cheese" architecture with myoepithelial-like cells, basement-membrane material, and perineural invasion — typical of salivary gland tumours, not oral SCC.
Teaching pearl: SCC differentiation grading (Broders):
| Grade | Differentiation | Keratin pearls | Mitoses | Cell borders |
|---|
| Grade 1 (well-differentiated) | Closely resembles normal squamous epithelium | Numerous | Few | Distinct, intercellular bridges |
| Grade 2 (moderately) | Some recognisable keratinisation | Some | Moderate | Mostly distinct |
| Grade 3 (poorly) | Difficult to recognise as squamous | Rare or absent | Numerous, atypical | Indistinct |
| Grade 4 (undifferentiated) | No keratinisation | None | Many bizarre | Indistinct, single cells |
Common sites and risk factors:
- Skin — UV exposure, immunosuppression (organ transplant), HPV
- Oral cavity — tobacco (smoked + smokeless), alcohol, betel nut, HPV (especially oropharyngeal HPV-16)
- Lung (central) — smoking; cavitates, central tumour, hypercalcemia from PTHrP
- Cervix — HPV-16, HPV-18; precursor is CIN
- Esophagus — alcohol, hot drinks, achalasia, tylosis (familial)
- Larynx, Anal canal — smoking and HPV respectively
Clinical pearls: SCC of the lung produces PTHrP and causes hypercalcemia of malignancy; oral SCC commonly metastasises to cervical lymph nodes following neck levels; cervix SCC is staged with FIGO; cutaneous SCC has Mohs surgery as gold standard for high-risk lesions.
Common pitfalls — patterns that can be confused
Pitfall 1: Reed-Sternberg-like cells in non-Hodgkin lymphomas
CD30-positive anaplastic large cell lymphoma (ALCL) and CD30-positive subtypes of DLBCL can have RS-like cells. The polymorphous background of small reactive lymphocytes, eosinophils, and plasma cells favours classical Hodgkin lymphoma, while sheets of monomorphic large cells favour DLBCL or ALCL. Immunophenotype clinches: classic RS = CD30+ CD15+ CD20-; ALCL = CD30+ ALK+ (in pediatric); DLBCL = CD20+.
Pitfall 2: Psammoma bodies versus dystrophic calcifications
Psammoma bodies are concentric lamellated calcifications with onion-skin layering. They are different from amorphous dystrophic calcifications (e.g., in old infarcts) and from psammomatous calcium oxalate (in some thyroid lesions). The four-location list (PTC, serous ovarian, meningioma, papillary RCC) is the high-yield NEET PG association.
Pitfall 3: Auer rods in MDS versus AML
Auer rods can occasionally appear in high-grade myelodysplastic syndromes (MDS-EB-2 with Auer rods is a defined WHO category). Don't assume Auer rods = AML M3 always. Bundles (faggot cells) plus the bilobed nucleus and DIC clinical picture clinch APL.
Pitfall 4: Signet ring cells in benign mimics
Benign signet ring cell change is rarely seen in foveolar hyperplasia (Menetrier disease) and in some lymphangiectasis. True malignant signet ring cells are atypical, infiltrative, and produce desmoplasia. In peritoneal cytology, cytomorphology + immunohistochemistry (CK20, CDX2 for GI; ER, GCDFP-15 for breast) directs the primary search.
Pitfall 5: Keratin pearls in benign hyperkeratosis
Benign hyperkeratosis (lichen planus, frictional keratosis) shows surface orthokeratosis without invasive squamous nests in the deep tissue. Keratin pearls within infiltrating nests with desmoplasia and atypia confirm SCC. Dysplasia (CIN, oral epithelial dysplasia) is precursor; carcinoma in situ has full-thickness atypia without invasion through the basement membrane.
Frequently Asked Questions
Why are Reed-Sternberg cells the diagnostic hallmark of classical Hodgkin lymphoma?
Reed-Sternberg cells are large bi-nucleated or multi-nucleated B-cell-derived neoplastic cells with prominent eosinophilic owl-eye nucleoli. They are the defining cell of classical Hodgkin lymphoma — without them you cannot diagnose cHL. They are CD30 positive, CD15 positive, CD20 negative or weakly positive, CD45 negative, and PAX5 weakly positive. Variants include lacunar (nodular sclerosis subtype), mummified (apoptotic), pleomorphic (lymphocyte-depleted), and popcorn or LP cells (nodular lymphocyte-predominant Hodgkin lymphoma — CD20 positive, CD30 negative, CD15 negative).
Where do psammoma bodies appear and what is their significance?
Psammoma bodies are concentric lamellated calcium concretions resembling sand grains — the name is from the Greek psammos meaning sand. The classic four locations: papillary thyroid carcinoma, serous papillary cystadenocarcinoma of the ovary, meningioma (especially psammomatous variant), and papillary renal cell carcinoma. They are also seen in some mesotheliomas and prolactinomas. Mechanism is dystrophic calcification on apoptotic tumour cells. They support malignancy when present in ovarian or thyroid lesions but are not pathognomonic alone — context plus other features (Orphan Annie nuclei in PTC, complex papillary architecture) seals the diagnosis.
What are Auer rods and which leukemia do they identify?
Auer rods are needle-shaped crystalline cytoplasmic inclusions formed by fused azurophilic granules — visible on Wright-Giemsa-stained peripheral smear or bone marrow aspirate. They are pathognomonic of myeloid lineage and rule out lymphoid leukemia. Numerous Auer rods bundled together (faggot cells) are characteristic of acute promyelocytic leukemia (AML M3, t(15;17), PML-RARA). Single Auer rods are seen in AML M1, M2, M4, M5. APL is an oncological emergency: high risk of DIC, give all-trans retinoic acid (ATRA) plus arsenic trioxide as soon as the diagnosis is suspected, before molecular confirmation.
What is the typical context for signet ring cells on histology?
Signet ring cells are tumour cells with intracytoplasmic mucin pushing the nucleus to the periphery, mimicking a signet ring. The two classic primary sites: poorly cohesive (signet ring cell) carcinoma of the stomach (linitis plastica gives a leather-bottle appearance) and invasive lobular carcinoma of the breast (where signet ring cells lie in single-file Indian-file pattern; E-cadherin loss is the molecular hallmark). They also appear in colorectal adenocarcinoma and pulmonary mucinous adenocarcinoma. When seen in a peritoneal biopsy of a young woman, suspect Krukenberg tumour — bilateral ovarian metastasis from gastric primary.
What are keratin pearls and what tumour do they identify?
Keratin pearls (squamous pearls, epithelial pearls) are concentric whorls of squamous cells with central keratinisation — the histologic hallmark of well-differentiated squamous cell carcinoma. They reflect the tumour's attempt to recapitulate normal squamous epithelium. Common sites: skin, oral cavity, lung (especially central, smoking-related), cervix (HPV-driven), esophagus, larynx, anal canal. Key intercellular bridges are also visible at high power. The presence of numerous keratin pearls indicates well-differentiated SCC; their absence with poorly defined cell borders and high mitotic rate indicates poorly differentiated SCC.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: April 2026