## AAA Management: Surveillance vs. Repair Thresholds **Surveillance with imaging every 6 months** is the most appropriate strategy for this asymptomatic 5 cm AAA in a high-risk patient. ### Key Point: - **Repair threshold**: 5.5 cm (or 5.0 cm if rapid expansion >0.6 cm/year, female, or connective tissue disorder) - **Current size**: 5 cm—below the threshold for elective repair - **Risk stratification**: This patient has **high perioperative risk** (EF 35%, CKD Stage 3b, COPD) ### Evidence Base (UK Small Aneurysm Trial, ADAM Trial): - Elective repair at 5.5 cm offers survival benefit vs. surveillance - **Below 5.5 cm**: Surveillance is safer; rupture risk is low (~1% per year at 5 cm) - **High-risk patients**: Perioperative mortality from elective repair may exceed rupture risk ### Surveillance Protocol: - **AAA 4.0–4.9 cm**: Ultrasound annually - **AAA 5.0–5.4 cm**: Ultrasound every 6 months (or CT if anatomy unclear) - **Expansion >0.6 cm/year**: Consider repair even below 5.5 cm ### Clinical Pearl: In high-risk patients with comorbidities, **delaying elective repair** until 5.5 cm or until expansion accelerates reduces perioperative mortality without increasing rupture risk. 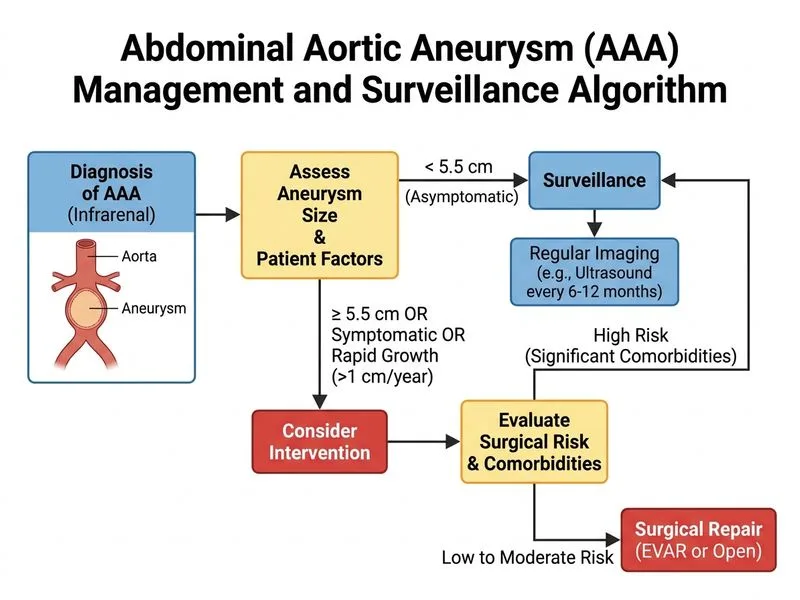
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.