## Diagnosis and Management of Acute Appendicitis ### Clinical Presentation This patient presents with the classic triad of acute appendicitis: 1. Periumbilical pain migrating to RLQ (visceral → somatic innervation) 2. Anorexia preceding nausea/vomiting (not the reverse) 3. Fever and leukocytosis with left shift ### Diagnostic Findings | Finding | Significance | |---------|-------------| | McBurney's point tenderness | Anatomical landmark at junction of lateral 1/3 and medial 2/3 of line from ASIS to umbilicus | | Rovsing's sign positive | RLQ pain on left lower quadrant palpation; indicates peritoneal irritation | | Guarding and rebound | Peritonitis present | | Ultrasound: non-compressible appendix >6 mm, wall >2 mm, periappendiceal fluid | Diagnostic criteria met for acute appendicitis | **Key Point:** In uncomplicated acute appendicitis with confirmed diagnosis on imaging, **immediate appendicectomy is the gold standard**. Delay increases risk of perforation (which occurs in ~25% of cases if untreated for >48 hours). **High-Yield:** The patient has no signs of perforation (no generalized peritonitis, no septic shock, no imaging evidence of abscess or free air), so emergency surgery is indicated without further delay. **Clinical Pearl:** Interval appendicectomy (antibiotics now, surgery in 6 weeks) is reserved for **perforated appendicitis with localized abscess** or **appendiceal mass** — not uncomplicated acute appendicitis. ### Why Immediate Surgery? - Uncomplicated acute appendicitis has near 100% cure rate with appendicectomy - Mortality <1% in uncomplicated cases; rises sharply if perforation occurs - Imaging diagnosis is already secure (ultrasound criteria met) - No contraindications to surgery in this young, stable patient [cite:Bailey & Love 28e Ch 71] 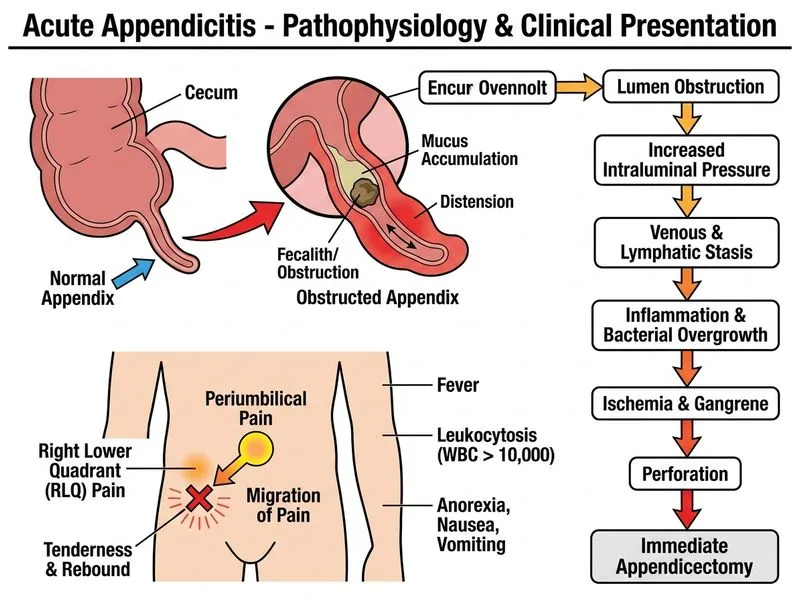
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.