## Management of Perforated Appendicitis with Localized Abscess ### Clinical Scenario Analysis This patient presents with: - **Perforated appendicitis** (imaging confirms perforation) - **Localized abscess** (well-defined 4 cm collection, no free air) - **Stable vital signs** (fever present but no septic shock) - **Palpable mass** (suggests walling off by omentum/peritoneum) ### Management Strategy: Percutaneous Drainage + Interval Appendicectomy ```mermaid flowchart TD A[Perforated Appendicitis]:::outcome --> B{Abscess present?}:::decision B -->|Yes, localized| C[Percutaneous drainage]:::action B -->|No, free perforation| D[Emergency appendicectomy]:::urgent C --> E[Antibiotics 5-7 days]:::action E --> F[Interval appendicectomy 6-8 weeks]:::action F --> G[Complete recovery]:::outcome D --> H[Source control + drainage]:::action ``` ### Rationale for Percutaneous Drainage First **Key Point:** In **perforated appendicitis with localized abscess**, the Ochsner-Sherren principle applies: **drain the abscess first, operate later**. This avoids spillage of infected material during immediate surgery. | Approach | Indication | Outcome | |----------|-----------|----------| | **Percutaneous drainage + interval appendicectomy** | Localized abscess, stable patient | Lower morbidity, faster recovery | | **Immediate appendicectomy** | Free perforation, peritonitis, unstable | Necessary for source control | | **Antibiotics alone** | Uncomplicated acute appendicitis | Incomplete; abscess will persist | **High-Yield:** The presence of a **well-defined abscess with no free air** is the key distinguishing feature. This indicates the patient's peritoneum has successfully walled off the infection — a favorable scenario for non-operative drainage. ### Step-by-Step Management 1. **Percutaneous drainage** (CT or ultrasound-guided) — removes infected fluid, relieves sepsis 2. **Broad-spectrum antibiotics** (e.g., ceftriaxone + metronidazole or piperacillin-tazobactam) for 5–7 days 3. **Supportive care** — IV fluids, analgesia, NPO status 4. **Interval appendicectomy** — performed 6–8 weeks after abscess resolution and clinical improvement - Allows inflammation to settle - Reduces operative bleeding and tissue friability - Lower recurrence risk compared to immediate surgery in this setting **Clinical Pearl:** If the abscess cannot be drained percutaneously (e.g., very small, inaccessible location), immediate appendicectomy may be necessary. However, in this case, a 4 cm well-defined collection is ideal for drainage. **Warning:** Do NOT attempt laparoscopic appendicectomy in the acute phase of perforated appendicitis with abscess — risk of abscess rupture and peritoneal contamination is high. [cite:Bailey & Love 28e Ch 71; Sabiston Textbook of Surgery 21e Ch 51] 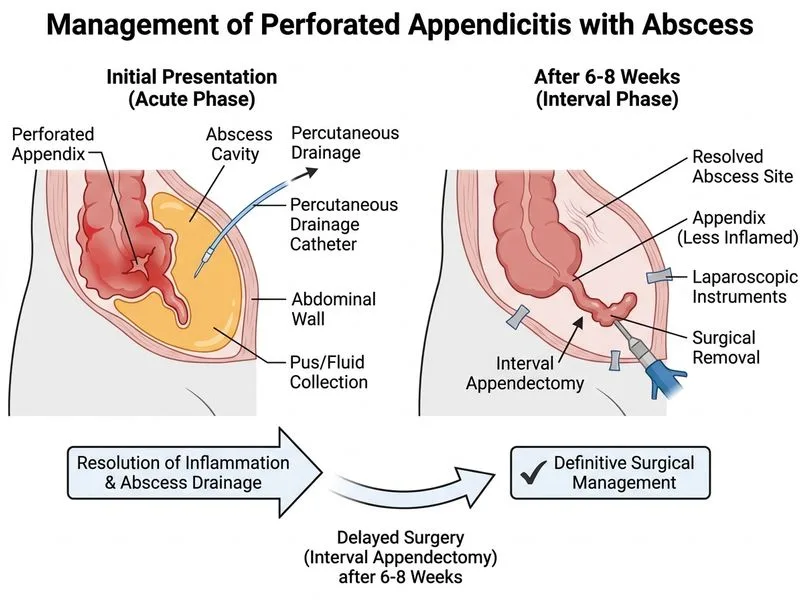
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.