## Diagnosis and Management of Acute Appendicitis ### Clinical Presentation **Key Point:** The classic triad of acute appendicitis is periumbilical pain migrating to the right lower quadrant, followed by anorexia and then vomiting (not vomiting first). This patient presents with textbook features: - Migration of pain from periumbilical region to RLQ - Anorexia preceding vomiting - Fever and systemic signs - Positive McBurney's point tenderness - Positive Rovsing's sign (pain in RLQ when palpating LLQ) - Elevated WBC with left shift ### Diagnostic Confirmation **High-Yield:** Ultrasound findings of a dilated (>6 mm), non-compressible appendix with periappendiceal free fluid are diagnostic of acute appendicitis. Further imaging (CT) is unnecessary when clinical and ultrasound findings are concordant. ### Definitive Management **Key Point:** Acute appendicitis is a surgical emergency. Once diagnosed, the standard of care is appendicectomy (open or laparoscopic) without delay. **Clinical Pearl:** Delayed appendicectomy increases the risk of perforation, peritonitis, and sepsis. This patient has no contraindications to surgery and no signs of perforation (yet), making immediate surgical intervention the gold standard. ### Why Immediate Surgery? 1. Diagnostic certainty achieved (clinical + ultrasound) 2. Risk of progression to perforation increases with time 3. No evidence of established perforation or peritonitis requiring preoperative optimization 4. Laparoscopic appendicectomy is safe and preferred when expertise available [cite:Sabiston Textbook of Surgery Ch 50] 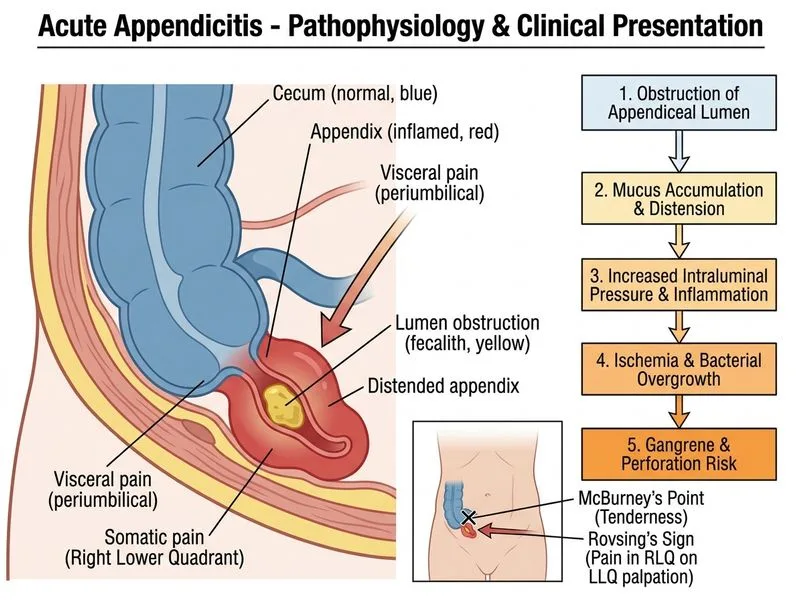
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.