## Management of Perforated Appendicitis with Localized Abscess ### Clinical Scenario Analysis **Key Point:** This patient has a **perforated appendix with a localized (contained) pelvic abscess** — a fundamentally different clinical situation from simple acute appendicitis or free perforation with diffuse peritonitis. The presence of a contained abscess changes the management paradigm entirely. ### Pathophysiology 1. Appendiceal perforation occurred (likely 48+ hours ago based on symptom duration) 2. Omentum and adjacent bowel loops have walled off the infection 3. A **localized abscess** has formed (4 cm — well-defined on CT) 4. This is a **contained perforation**, NOT diffuse peritonitis ### Distinguishing Contained Abscess from Diffuse Peritonitis | Feature | This Patient | Diffuse Peritonitis | |---------|-------------|---------------------| | Tenderness | Localized RLQ/pelvis | Generalized, board-like rigidity | | Hemodynamic status | Stable (no shock) | Often unstable | | CT findings | Localized abscess, walled off | Free air, free fluid throughout | | Management | Percutaneous drainage + interval appendicectomy | Emergency surgery | > **Important:** The guarding and rebound tenderness in this patient are **localized to the RLQ**, consistent with a contained process — not the generalized peritonitis that would mandate emergency surgery. The patient is hemodynamically stable with no mention of septic shock. ### Optimal Management Strategy: Percutaneous Drainage + Interval Appendicectomy **High-Yield (Sabiston / Bailey & Love):** For perforated appendicitis with a well-defined localized abscess (typically ≥3 cm), the standard of care is: | Phase | Timing | Intervention | Rationale | |-------|--------|--------------|-----------| | **Acute** | Day 0–3 | CT/US-guided percutaneous drainage + IV broad-spectrum antibiotics | Resolves abscess, reduces inflammation, stabilizes patient | | **Interval** | Week 6–8 | Elective appendicectomy | Performed after inflammation subsides — lower morbidity, safer dissection | ### Why NOT Immediate Surgery (Options A or B)? **Clinical Pearl:** Immediate appendicectomy in the setting of a localized abscess carries significant risks: - **Spillage of pus** into the peritoneal cavity converting contained to diffuse peritonitis - **Obliterated tissue planes** due to severe inflammation — increased risk of bowel/vascular injury - Higher rates of wound infection, ileus, and anastomotic complications - Laparoscopic approach (Option B) carries additional risk of abscess rupture during dissection and pneumoperitoneum-related spread of contamination ### Why NOT Antibiotics Alone (Option C)? - A **4 cm abscess** requires drainage for source control; antibiotics alone are insufficient for abscesses >3 cm - Risk of treatment failure, recurrence, and systemic sepsis without drainage - Antibiotics alone may be considered for phlegmon (no discrete abscess) but not for a well-defined abscess cavity ### Role of Serum Creatinine (1.4 mg/dL) **Key Point:** The mildly elevated creatinine likely reflects **early sepsis-related acute kidney injury (AKI)** or pre-renal azotemia from vomiting/dehydration. This further supports a non-operative initial approach — aggressive IV fluid resuscitation alongside percutaneous drainage is safer than subjecting a patient with early renal impairment to emergency surgery under general anesthesia. ### Antibiotic Coverage Broad-spectrum antibiotics covering gram-negative organisms and anaerobes are essential: - **Piperacillin-tazobactam** (monotherapy), OR - **Ceftriaxone + Metronidazole** (combination) Continue until clinical improvement and abscess resolution confirmed on imaging. **High-Yield:** The interval appendicectomy rate after conservative management is approximately 20–30% (many patients never develop recurrence), but elective surgery at 6–8 weeks remains the standard recommendation to prevent recurrent appendicitis. [cite: Sabiston Textbook of Surgery, 20th Ed., Ch. 50; Bailey & Love's Short Practice of Surgery, 27th Ed.] 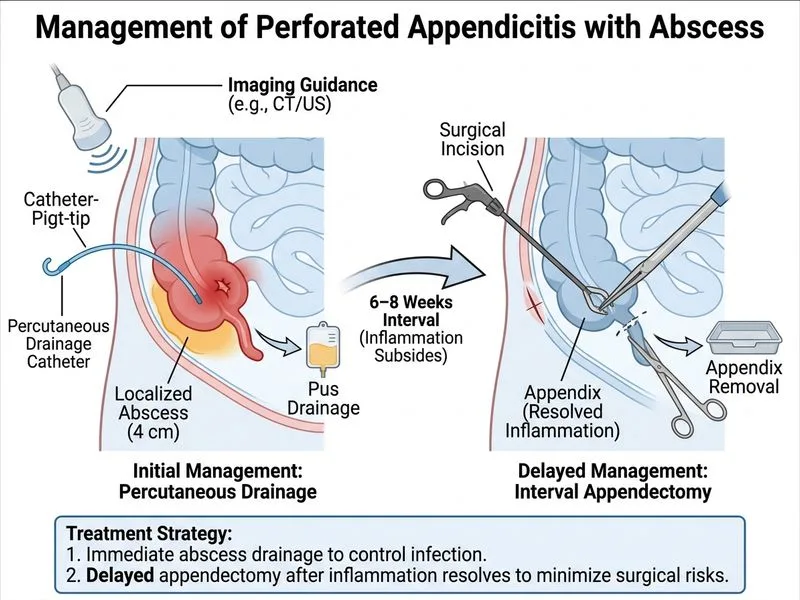
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.