Acute Leukemias MCQ — NEET PG Practice Question | NEETPGAI
Acute Leukemias
medium
microscope Pathology
A 28-year-old woman from Delhi presents with a 3-week history of progressive fatigue, fever, and spontaneous bruising. On examination, she is pale with petechiae and hepatosplenomegaly. Laboratory findings show: Hb 7.2 g/dL, WBC 45,000/μL (70% blasts), platelets 18,000/μL. Bone marrow examination reveals >80% blasts with Auer rods. Flow cytometry shows CD13+, CD33+, MPO+, HLA-DR+. What is the most likely diagnosis?
The patient presents with the classic triad of APL:
1.
Severe thrombocytopenia (18,000/μL) — often <50,000/μL
2.
Coagulopathy — spontaneous bruising and petechiae
3.
High-risk bleeding — DIC is the hallmark complication
Morphologic & Immunophenotypic Features
Table
Feature
APL (M3)
Finding in this case
Auer rods
Pathognomonic; often multiple ("faggot cells")
Present ✓
Blast morphology
Abnormal promyelocytes with heavy granulation
Consistent with morphology
Immunophenotype
CD13+, CD33+, MPO+, HLA-DR+ (or −)
Matches ✓
Cytogenetics
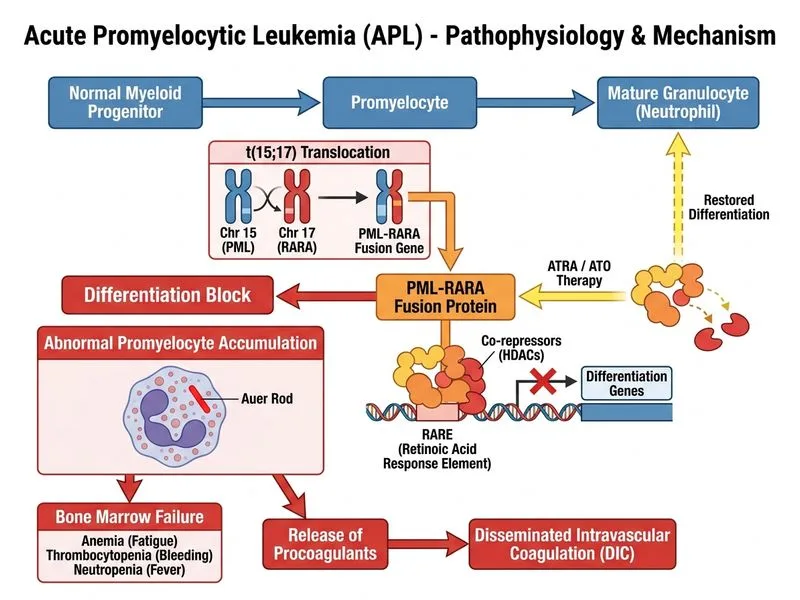
t(15;17) — PML-RARA fusion
Gold standard (not given but diagnostic)
Coagulopathy
DIC due to release of tissue factor from leukemic cells
Explains bruising/petechiae
Key Point
Auer rods are most abundant and characteristic in APL; multiple Auer rods in a single cell ("faggot cells") are virtually pathognomonic for M3.
Why This Is APL and Not Other Subtypes
High-YieldNEET PG
APL is the only AML subtype where morphology + cytochemistry + immunophenotype + Auer rods converge to give a diagnosis. The presence of multiple Auer rods is the morphologic smoking gun.
Clinical Significance
Clinical Pearl
APL is a medical emergency due to:
DIC (disseminated intravascular coagulation) — caused by release of procoagulants (tissue factor, cancer procoagulant) from abnormal promyelocytes
Bleeding risk — spontaneous intracranial hemorrhage, GI bleed, pulmonary hemorrhage
Treatment response — APL is the most curable acute leukemia (>90% CR rate) with ATRA (all-trans retinoic acid) + arsenic trioxide; early recognition is life-saving