## Acute Limb Ischemia: Emergency Management ### Clinical Presentation Recognition This patient presents with the classic **6 Ps of acute limb ischemia**: Pain, Pallor, Pulselessness, Paresthesia, Paralysis (sensory loss), and Perishing cold. The 3-hour duration places this in the **hyperacute phase** (0–6 hours), where tissue is still viable and salvageable. **Key Point:** Acute limb ischemia is a vascular emergency. Delays >6–8 hours result in irreversible muscle necrosis and gangrene. ### Why Immediate Heparin + Surgical Consultation? **High-Yield:** The source of embolism in this case is almost certainly the patient's **atrial fibrillation** (cardioembolic source). Immediate anticoagulation with IV heparin prevents propagation of thrombus and buys time for definitive intervention. **Clinical Pearl:** In acute limb ischemia with sensory loss but preserved motor function (Rutherford Category IIa–IIb), the limb is still salvageable. Urgent vascular surgery consultation for embolectomy (Fogarty catheter) or endovascular thrombectomy is the standard of care. ### Rutherford Classification of Acute Limb Ischemia | Category | Sensory Loss | Motor Loss | Muscle Tenderness | Viability | |----------|--------------|------------|-------------------|----------| | I (Viable) | None | None | None | Viable | | IIa (Threatened, marginal) | Minimal | None | None | Salvageable | | IIb (Threatened, immediate) | Sensory + motor | Minimal | None | Salvageable | | III (Irreversible) | Profound | Profound | Yes | Not salvageable | **Key Point:** This patient is **Category IIa–IIb** (sensory loss present, no mention of motor loss yet). The limb is still salvageable with urgent intervention. ### Management Algorithm ```mermaid flowchart TD A[Acute limb ischemia diagnosis]:::outcome --> B[Start IV heparin immediately]:::action B --> C[Urgent vascular surgery consult]:::action C --> D{Rutherford category?}:::decision D -->|Category I| E[Observation, anticoagulation]:::action D -->|Category IIa-IIb| F[Embolectomy or endovascular thrombectomy]:::action D -->|Category III| G[Amputation consideration]:::urgent F --> H[Reperfusion achieved]:::outcome ``` **Mnemonic:** **HALT** — **H**eparin, **A**ngiography/Assessment, **L**ower limb assessment (Rutherford), **T**herapy (surgery/endovascular). ### Why NOT the Other Options? - **Aspirin alone + duplex tomorrow:** Aspirin is too slow; the limb will be gangrenous by morning. Duplex is not urgent enough for acute ischemia. - **Thrombolysis:** Systemic thrombolysis (alteplase) is contraindicated in acute embolic limb ischemia because (1) it is slower than mechanical embolectomy, (2) it carries high bleeding risk, and (3) the patient has atrial fibrillation (potential cardioembolic source requiring urgent mechanical removal). - **Warm compresses + warfarin:** Warming increases metabolic demand in ischemic tissue and worsens necrosis. Oral warfarin is far too slow; IV heparin is needed immediately. **Clinical Pearl:** Thrombolysis may be considered for acute thrombotic (not embolic) occlusion in a native artery with no sensory/motor loss, but embolectomy is faster and preferred in this acute presentation. [cite:Sabiston Textbook of Surgery 21e Ch 64] 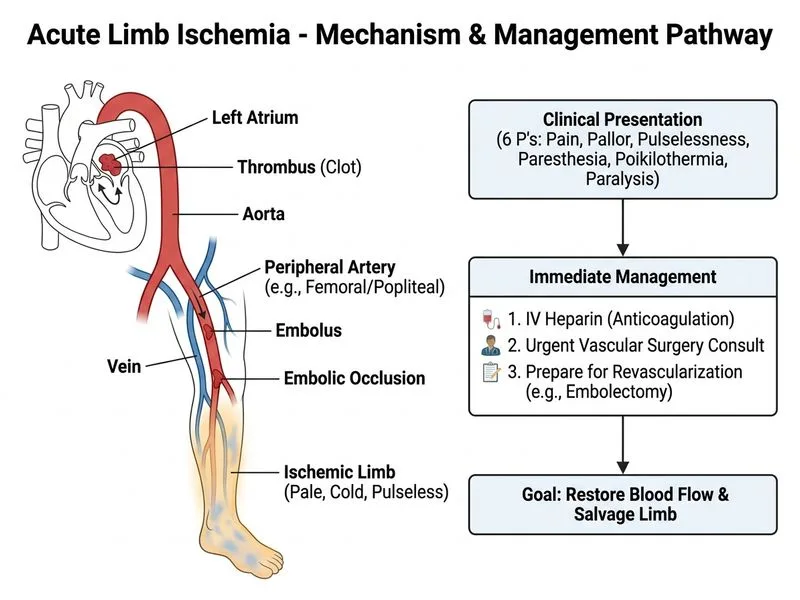
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.