## Acute Limb Ischemia: Thrombotic vs. Embolic Pathways ### Clinical Distinction This patient presents with **acute thrombotic limb ischemia** (not embolic), evidenced by: - **Underlying atherosclerotic disease** (diabetes, hypertension, likely chronic PAD) - **Thrombosis of a native artery** (SFA) rather than embolic occlusion - **Preserved proximal pulses** (femoral pulse present) with distal occlusion - **No cardiac source** (no mention of atrial fibrillation or recent MI) **Key Point:** Acute thrombosis on chronic atherosclerotic disease differs from acute embolism. The management strategy differs accordingly. ### Rutherford Viability Assessment This patient is **Rutherford Category I (Viable)**: no sensory loss, no motor deficit, no muscle tenderness, and within 12 hours of onset. The limb is currently viable but at risk. **High-Yield:** In viable acute limb ischemia (Category I), the goal is to restore perfusion while preserving the limb. The choice between thrombolysis, thrombectomy, or hybrid approaches depends on: 1. **Duration of ischemia** (12 hours is still within the window) 2. **Viability status** (this patient is viable) 3. **Availability of intervention** (endovascular vs. surgical) 4. **Underlying anatomy** (native artery thrombosis) ### Management Algorithm for Acute Thrombotic Limb Ischemia ```mermaid flowchart TD A[Acute thrombotic limb ischemia]:::outcome --> B[IV heparin immediately]:::action B --> C[Assess Rutherford category]:::decision C -->|Category I: Viable| D[Thrombolysis vs. Thrombectomy?]:::decision C -->|Category IIa-IIb: Threatened| E[Urgent intervention needed]:::action C -->|Category III: Irreversible| F[Amputation]:::urgent D -->|Early presentation, no contraindications| G[Catheter-directed thrombolysis]:::action D -->|Late presentation or lysis contraindication| H[Surgical/endovascular thrombectomy]:::action G --> I[Reperfusion + anticoagulation]:::outcome H --> I ``` ### Why Heparin + Thrombolysis Candidacy Assessment? **Clinical Pearl:** In acute thrombotic limb ischemia with viable tissue (Category I), **catheter-directed thrombolysis (CDT)** is often preferred over immediate surgery because: 1. It preserves native artery anatomy 2. It allows identification of underlying stenosis for subsequent PTA/stent 3. It has lower morbidity than surgical thrombectomy in viable limbs 4. This patient is within 12 hours (still within thrombolysis window) **Mnemonic:** **VITAL** — **V**iable limb, **I**schemia acute, **T**hrombolysis candidate, **A**nticoagulate, **L**ower limb salvage. ### Thrombolysis vs. Thrombectomy: When to Choose Each | Feature | Catheter-Directed Thrombolysis | Surgical Thrombectomy | |---------|--------------------------------|----------------------| | **Best for** | Viable limb, native artery, <12 hrs | Irreversible ischemia, embolic source, failed lysis | | **Advantage** | Preserves artery, identifies stenosis | Faster, definitive in emboli | | **Disadvantage** | Takes 12–24 hrs, bleeding risk | Invasive, may need amputation | | **Contraindications** | Recent surgery, active bleeding, stroke | Irreversible tissue loss | **Key Point:** This patient is a **thrombolysis candidate** (viable, within 12 hours, native artery thrombosis). Heparin + urgent vascular surgery consultation allows assessment for CDT vs. thrombectomy based on local expertise and contraindications. ### Why NOT the Other Options? - **Immediate thrombectomy:** While thrombectomy is an option, thrombolysis is often preferred in viable acute thrombotic occlusion because it preserves artery anatomy and identifies underlying stenosis. Immediate surgery is reserved for irreversible ischemia or failed thrombolysis. - **PTA with stent:** PTA/stenting is a secondary intervention performed **after** thrombolysis to treat the underlying stenosis that caused thrombosis. It is not the first-line acute intervention. - **Amputation:** Amputation is reserved for **irreversible ischemia (Category III)** with muscle necrosis and sepsis risk. This patient is viable and has no indication for amputation. **Clinical Pearl:** The underlying cause of thrombosis in this patient is likely atherosclerotic stenosis of the SFA. After successful thrombolysis, PTA ± stent will be needed to prevent re-thrombosis. [cite:Sabiston Textbook of Surgery 21e Ch 64; Harrison 21e Ch 297] 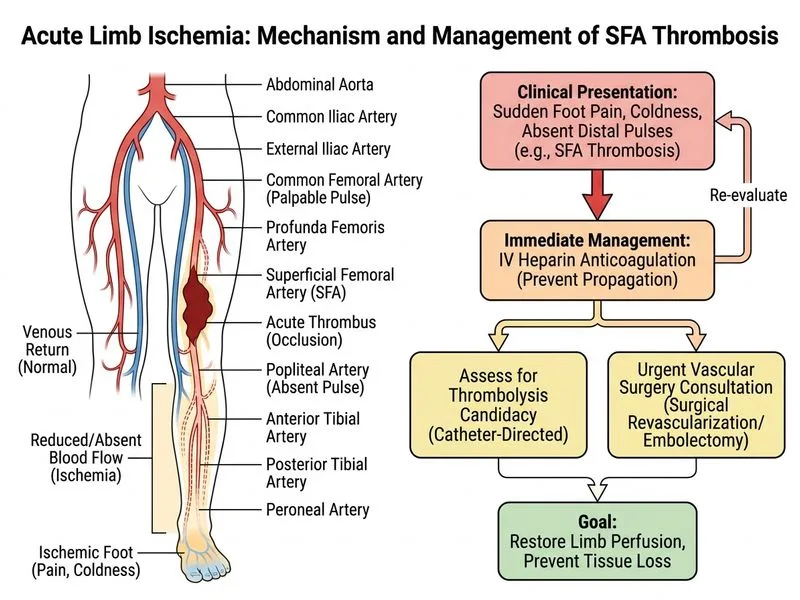
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.