## Acute Limb Ischemia: Clinical Presentation and Management ### Diagnosis This patient presents with **acute limb ischemia (ALI)** secondary to **arterial embolism** from atrial fibrillation. The classic presentation includes the **6 Ps**: Pain, Pallor, Pulselessness, Paresthesia, Paralysis, and Poikilothermia (coldness). **Key Point:** The sudden onset (2 hours) with absent pulses and preserved sensation indicates **acute arterial occlusion**, most likely embolic in origin given the AF history. ### Rutherford Classification This patient has **Category IIa (Viable limb with salvageable tissue)** — sensation intact, no motor loss, viable muscle. | Rutherford Grade | Sensory Loss | Motor Loss | Muscle Tenderness | Prognosis | |---|---|---|---|---| | I (Viable) | None | None | None | Salvageable | | IIa (Threatened, salvageable) | None | None | None | Salvageable with intervention | | IIb (Threatened, marginally salvageable) | Minimal | Minimal | None | Salvageable with aggressive intervention | | III (Irreversible) | Absent | Absent | Present | Amputation inevitable | ### Management Algorithm ```mermaid flowchart TD A[Acute Limb Ischemia Suspected]:::outcome --> B{Time since onset?}:::decision B -->|< 6 hours| C[Immediate IV heparin bolus]:::action B -->|6-14 hours| C C --> D{Viable limb?}:::decision D -->|Yes| E[Urgent vascular surgery consult]:::action E --> F{Embolic source?}:::decision F -->|Yes - AF, cardiac| G[Surgical embolectomy]:::action F -->|No - thrombotic| H[Consider thrombolysis or thrombectomy]:::action D -->|No - irreversible| I[Amputation]:::urgent G --> J[Reperfusion achieved]:::outcome ``` **High-Yield:** Immediate IV **heparin** (bolus 5000 IU, then 1000 IU/hr) is the first-line anticoagulation to prevent thrombus propagation and buy time for definitive intervention. ### Why Embolectomy? 1. **Embolic source identified** — atrial fibrillation is a cardioembolic source 2. **Short symptom duration** (2 hours) — tissue still viable 3. **Surgical embolectomy** (Fogarty catheter) is the gold standard for acute emboli with viable limbs 4. **Speed matters** — every hour increases tissue loss risk **Clinical Pearl:** The presence of intact sensation and no motor loss indicates the limb is still salvageable. Delay in intervention beyond 6–8 hours significantly increases amputation risk. **Warning:** Do NOT observe or delay — acute limb ischemia is a surgical emergency. Waiting for symptoms to resolve is dangerous and leads to irreversible tissue loss. ### Why Not Thrombolysis? While thrombolysis (alteplase, urokinase) can be used in acute limb ischemia, it is **NOT first-line for embolic occlusions** with a clear cardiac source. Thrombolysis is preferred for: - Native arterial thrombosis (atherosclerotic) - Graft thrombosis - Symptom duration 6–14 hours - Borderline viable limbs Embolectomy is faster and more reliable for emboli. 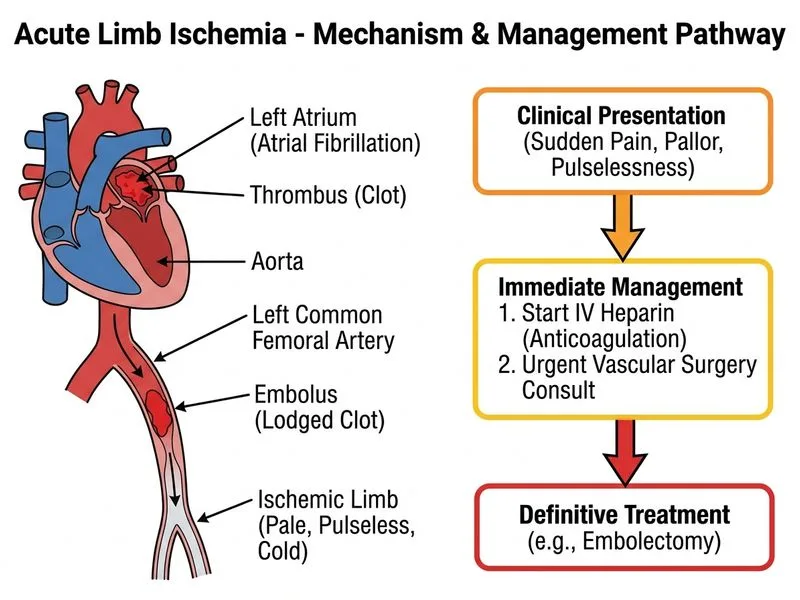
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.