In acute suppurative otitis media, bacterial infection (commonly Streptococcus pneumoniae, Haemophilus influenzae, or Moraxella catarrhalis) causes:
| Indication | Rationale |
|---|---|
| Bulging TM under tension | Pressure relief; prevents spontaneous traumatic perforation |
| Severe pain (3 days) | Immediate symptom relief — antibiotics take 24–48 hrs to act |
| Impending perforation | Controlled drainage vs. uncontrolled rupture |
| Fever + toxicity in child | Rapid source control; pus available for culture |
Clinical Pearl (Scott-Brown's Otolaryngology): Myringotomy is a therapeutic procedure in ASOM with a bulging TM. It provides immediate pain relief, prevents spontaneous perforation, and allows bacteriological sampling. It is the standard of care when the TM is under tension.
Important nuance (SME-flagged): In a 4-year-old child, myringotomy under local anesthesia alone is technically challenging due to lack of cooperation. In clinical practice, myringotomy in young children is typically performed under general anesthesia or with appropriate sedation. The option states "under local anesthesia," which reflects the procedural label used in many Indian PG textbooks (Dhingra's ENT); for NEET PG purposes, myringotomy remains the correct answer regardless of anesthetic modality.
Reference: Dhingra PL, Diseases of Ear, Nose and Throat, 7th ed.; Scott-Brown's Otolaryngology, 8th ed. — Myringotomy is indicated in ASOM when the TM is bulging and under tension.
Loading illustration…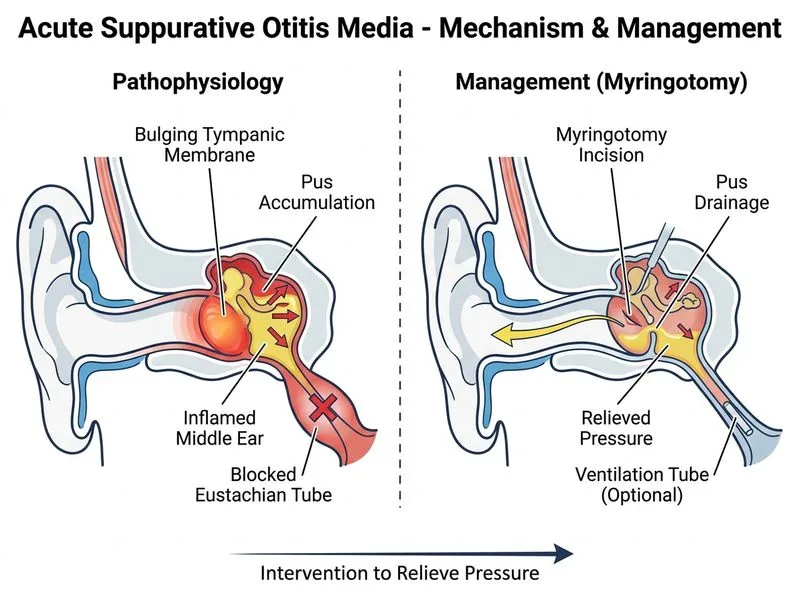
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →