Acute Suppurative Otitis Media MCQ — NEET PG Practice Question | NEETPGAI
Acute Suppurative Otitis Media
medium
ear ENT
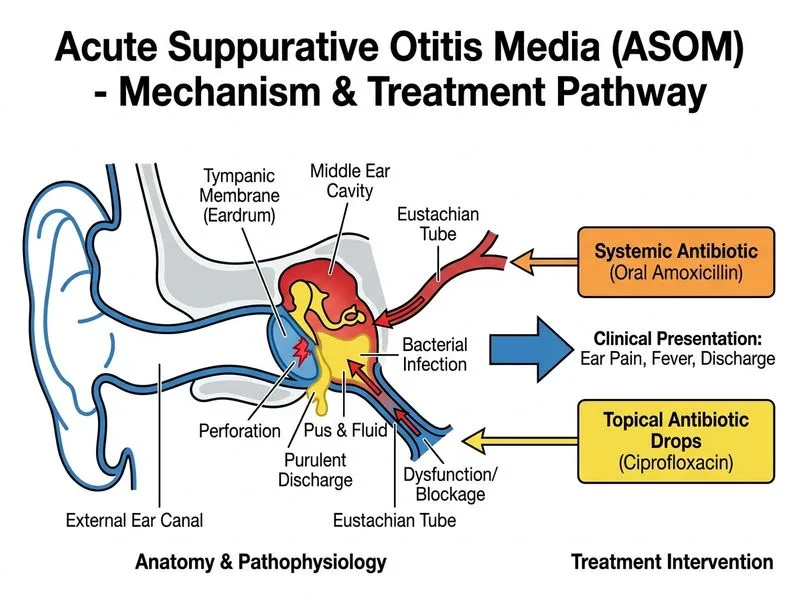
A 3-year-old girl from Delhi presents with right ear pain and fever for 5 days. Otoscopy shows a purulent discharge draining from the ear canal and a perforated tympanic membrane. The child has already received oral amoxicillin for 3 days without improvement. Systemic examination reveals no mastoid tenderness, no facial nerve involvement, and normal hearing in the left ear. What is the most appropriate next step in management?
A. Perform mastoidectomy and explore for complications
B. Switch to intravenous ceftriaxone and admit for observation
C. Perform myringoplasty under general anaesthesia
D. Continue oral amoxicillin and add topical antibiotic ear drops (ciprofloxacin)
Explanation
Clinical Scenario Analysis
This child has acute suppurative otitis media with spontaneous perforation and otorrhea — a sign that the infection has "drained" and pressure has been relieved. Despite 3 days of oral amoxicillin, discharge persists, indicating either:
1.
Inadequate oral antibiotic penetration into the middle ear space, OR
2.
Resistant organism.
Management of ASOM with Perforation and Otorrhea
Key Point
When acute otitis media perforates with active otorrhea, the combination of oral antibiotics + topical antibiotic ear drops is the standard first-line approach Park 26e Ch 5.
Rationale
1.
Topical antibiotics achieve high middle ear concentration via direct application to the perforation site, bypassing the need for systemic penetration.
2.
Fluoroquinolone drops (ciprofloxacin, ofloxacin) are preferred because they:
Penetrate biofilm in the middle ear
Cover common pathogens (Streptococcus pneumoniae, Haemophilus influenzae, Moraxella, Pseudomonas)
Are safe for use in perforated tympanum (unlike aminoglycosides, which are ototoxic)
3.
Oral antibiotics should be continued or escalated (e.g., amoxicillin-clavulanate or second-generation cephalosporin) to address systemic infection.
4.
Observation for 48–72 hours after starting this regimen is standard; most cases resolve without further intervention.
Clinical Pearl
Spontaneous perforation is often a favorable prognostic sign — it relieves middle ear pressure and allows drainage. Most children recover uneventfully with conservative management. Perforation usually heals spontaneously within 2–4 weeks.
Suspect mastoiditis → IV antibiotics + imaging (CT)
Facial nerve palsy
Urgent ENT referral; consider IV antibiotics
Meningeal signs (neck stiffness, photophobia)
Suspect meningitis → IV antibiotics + lumbar puncture
Persistent fever > 48 hrs despite IV antibiotics
Imaging (CT mastoid) to rule out abscess/complications
Cholesteatoma or chronic suppuration
Surgical consultation
High-YieldNEET PG
In this case, no mastoid tenderness, no facial nerve involvement, and normal contralateral hearing rule out complications. Topical + oral antibiotics are appropriate. Myringoplasty is premature (wait 3 months post-perforation for spontaneous healing). Mastoidectomy is not indicated without evidence of mastoiditis.
Antibiotic Selection for Otorrhea
Table
Drug
Advantages
Disadvantages
Ciprofloxacin drops
Broad spectrum, biofilm penetration, safe in perforation
Cost, resistance in some regions
Ofloxacin drops
Similar to ciprofloxacin
Similar
Gentamicin drops
Cheap, effective
Ototoxic — avoid in perforation
Chloramphenicol drops
Broad spectrum
Poor biofilm penetration
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.