A 52-year-old man from Delhi presents with a 6-month history of progressive abdominal distension, ankle swelling, and easy bruising. He reports consuming 80–100 g of alcohol daily for the past 15 years. On examination, he has jaundice, spider angiomas on the chest, palmar erythema, and a firm, enlarged liver edge 4 cm below the costal margin. Ascites is present. Laboratory findings: AST 280 U/L, ALT 95 U/L, ALP 210 U/L, bilirubin 4.2 mg/dL, albumin 2.8 g/dL, INR 2.1. Abdominal ultrasound shows cirrhotic echotexture with portal vein diameter 15 mm. What is the most likely histopathological finding in this patient's liver?
A. Bridging fibrosis with regenerative nodules and loss of normal architecture
B. Microvesicular steatosis with hepatocyte ballooning and minimal fibrosis
C. Acute hepatitis with portal inflammation and interface hepatitis only
D. Hepatic steatosis with acute inflammation and Mallory–Denk bodies
Explanation
Histopathological Diagnosis of Alcoholic Cirrhosis
Clinical Context
This patient presents with decompensated cirrhosis secondary to chronic alcohol use:
Markedly elevated AST >> ALT (characteristic of cirrhosis)
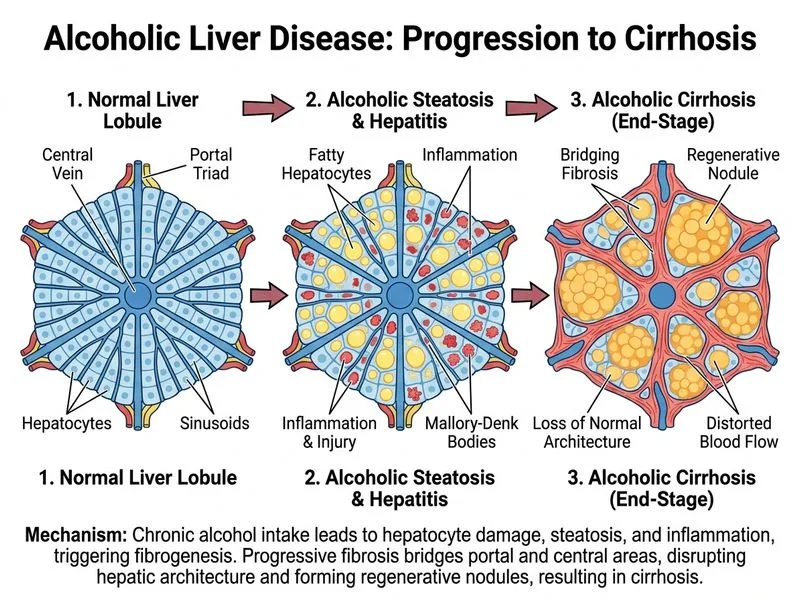
At this stage, the liver shows:
1.
Bridging fibrosis — fibrosis connecting portal tracts and bridging to central veins
2.
Regenerative nodules — islands of regenerating hepatocytes separated by fibrous septa
3.
Loss of normal architecture — obliteration of the normal hepatic lobular pattern
4.
Possible Mallory–Denk bodies (though less prominent in established cirrhosis than in acute alcoholic hepatitis)
High-YieldNEET PG
Cirrhosis is defined histologically as diffuse fibrosis with nodular regeneration and architectural distortion, not merely the presence of Mallory–Denk bodies or steatosis.
Why the Other Options Are Wrong
Option 0 (Hepatic steatosis with acute inflammation and Mallory–Denk bodies):
This describes acute alcoholic hepatitis, an earlier stage
Mallory–Denk bodies are prominent in acute hepatitis but less conspicuous in cirrhosis
Acute hepatitis is reversible; this patient has irreversible cirrhosis
Option 2 (Microvesicular steatosis with hepatocyte ballooning and minimal fibrosis):
Microvesicular steatosis is rare in alcoholic liver disease (more typical of acute fatty liver of pregnancy, drug toxicity)
"Minimal fibrosis" contradicts the imaging and clinical evidence of cirrhosis
This pattern would not produce portal hypertension
Option 3 (Acute hepatitis with portal inflammation and interface hepatitis only):
Describes chronic hepatitis without cirrhosis
Interface hepatitis (inflammation at the portal–parenchymal boundary) is seen in earlier stages
Does not explain the architectural distortion, nodules, or portal hypertension evident in this patient
Clinical Pearl
The AST:ALT ratio > 2 in alcoholic liver disease is a hallmark finding and reflects mitochondrial damage; it becomes more pronounced as cirrhosis develops. This patient's AST 280 vs. ALT 95 (ratio ~3) is classic for advanced alcoholic liver disease.
Mnemonic: ABCD of Alcoholic Liver Disease Progression