A 48-year-old woman from Mumbai with a 12-year history of heavy alcohol consumption (60–80 g/day) presents with acute onset of fever, right upper quadrant pain, and jaundice. She denies recent viral prodrome. Laboratory findings: WBC 14,500/μL, AST 520 U/L, ALT 180 U/L, ALP 320 U/L, bilirubin 6.8 mg/dL, albumin 2.9 g/dL, INR 1.8, prothrombin time 18 seconds. Serum markers for hepatitis A, B, and C are negative. Abdominal ultrasound shows hepatomegaly with coarse echotexture and ascites. A liver biopsy is performed. Which of the following histological findings would be most specific for the acute exacerbation of her underlying chronic alcoholic liver disease?
A. Bile duct proliferation with cholestasis and portal fibrosis
B. Granulomatous inflammation with caseating necrosis
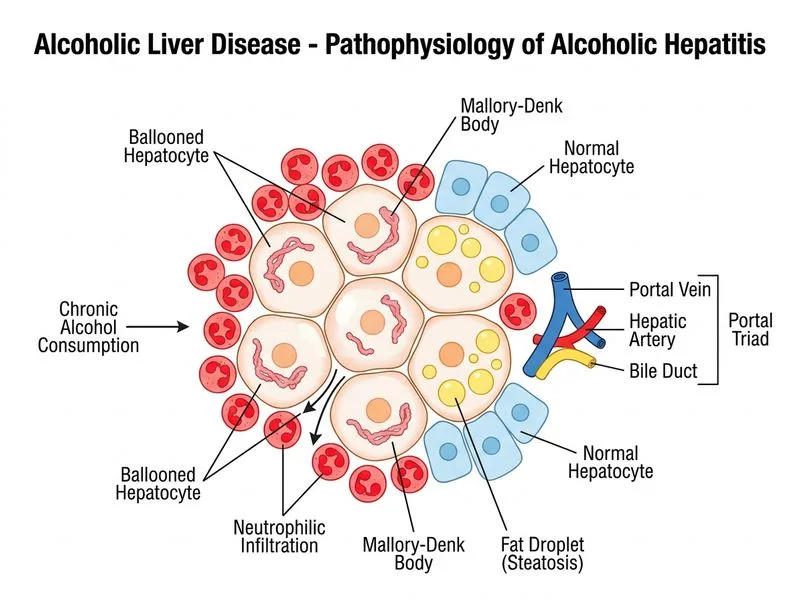
C. Neutrophilic infiltration around hepatocytes with Mallory–Denk bodies and hepatocyte ballooning
D. Microvesicular steatosis with mitochondrial inclusions and minimal inflammation
This patient presents with acute alcoholic hepatitis superimposed on chronic alcoholic liver disease:
Acute symptoms: Fever, RUQ pain, jaundice (onset over days)
Biochemical pattern: Marked elevation of AST (520) >> ALT (180), AST:ALT ratio ~3
Synthetic dysfunction: Elevated INR (1.8), low albumin (2.9 g/dL)
Inflammatory response: Leukocytosis (14,500/μL)
Exclusion of viral hepatitis: Negative serology for HAV, HBV, HCV
Imaging: Hepatomegaly with coarse echotexture and ascites (suggests underlying cirrhosis)
Histopathology of Acute Alcoholic Hepatitis
Key Point
Acute alcoholic hepatitis is characterized by a triad of findings:
Table
Finding
Description
Specificity
Neutrophilic infiltration
Polymorphonuclear leukocytes surrounding hepatocytes and in the portal tracts
High — hallmark of acute alcoholic hepatitis
Mallory–Denk bodies
Cytoplasmic inclusions of denatured proteins (ubiquitin, keratin) staining with orcein or trichrome
Specific but not pathognomonic (also seen in Wilson disease, NAFLD, PBC)
Hepatocyte ballooning
Swollen, pale hepatocytes with rarefied cytoplasm due to steatosis and cellular injury
Indicates acute hepatocellular injury
Macrovesicular steatosis
Large lipid droplets displacing the nucleus
Common but not specific
Cholestasis
Bile plugs in canaliculi and hepatocytes
Variable; more prominent in severe cases
Why Option 0 is Correct
High-YieldNEET PG
The neutrophilic infiltration around hepatocytes (also called "satellitosis") is the most specific histological finding for acute alcoholic hepatitis. This pattern is:
Characteristic of the acute inflammatory phase
Associated with hepatocyte necrosis and injury
Correlates with clinical severity and prognosis
When combined with Mallory–Denk bodies and hepatocyte ballooning, this triad is diagnostic of acute alcoholic hepatitis.
Clinical Pearl
The Maddrey discriminant function (DF) predicts prognosis in acute alcoholic hepatitis:
DF=(PTpatient−PTcontrol)×4.6+Bilirubin(mg/dL)
If DF > 32, mortality is high (~35%), and corticosteroid therapy may be considered. This patient's elevated INR and bilirubin suggest significant disease.
Why the Other Options Are Wrong
Option 1 (Microvesicular steatosis with mitochondrial inclusions and minimal inflammation):
Microvesicular steatosis is rare in alcoholic liver disease; it is characteristic of acute fatty liver of pregnancy, reye syndrome, and certain drug toxicities (valproate, tetracycline)
Alcoholic liver disease produces macrovesicular steatosis, not microvesicular
Minimal inflammation contradicts the acute presentation and leukocytosis
Option 2 (Granulomatous inflammation with caseating necrosis):
This pattern is seen in tuberculosis, sarcoidosis, fungal infections, and drug reactions
Granulomatous hepatitis is not a feature of alcoholic liver disease
Caseating granulomas would suggest tuberculosis or fungal disease, which are excluded by the clinical context
Option 3 (Bile duct proliferation with cholestasis and portal fibrosis):
Bile duct proliferation is a feature of cholestasis (from biliary obstruction, PBC, PSC, or drug-induced liver injury)
While cholestasis can occur in severe alcoholic hepatitis, it is not the specific hallmark
Portal fibrosis is a feature of chronic alcoholic liver disease, not the acute exacerbation
M — Mallory–Denk bodies (orcein-positive cytoplasmic inclusions)
A — Acute neutrophilic infiltration (satellitosis)
D — Diffuse macrovesicular steatosis
Warning
Do not confuse acute alcoholic hepatitis (acute inflammatory phase) with cirrhosis (chronic fibrotic end-stage). This patient likely has both: acute alcoholic hepatitis superimposed on underlying cirrhosis (evidenced by ascites, coarse echotexture, and low albumin). The biopsy will show both acute inflammation and chronic fibrosis.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.