A 48-year-old male from Delhi with a 20-year history of daily alcohol consumption presents with jaundice, ascites, and hepatic encephalopathy (Grade II). Laboratory investigations show: INR 2.8, total bilirubin 6.2 mg/dL, albumin 2.1 g/dL, platelet count 65,000/μL, and AST/ALT ratio 3.2. Ultrasound shows cirrhotic liver with portal vein diameter 14 mm. What is the most appropriate next step in management?
A. Supportive care with lactulose, rifaxomicin, and nutritional support; assess transplant candidacy
B. Start ursodeoxycholic acid and arrange outpatient follow-up in 2 weeks
C. Initiate corticosteroid therapy and pentoxifylline for alcoholic hepatitis
D. Immediate liver transplant evaluation and referral to transplant centre
Explanation
Clinical Assessment
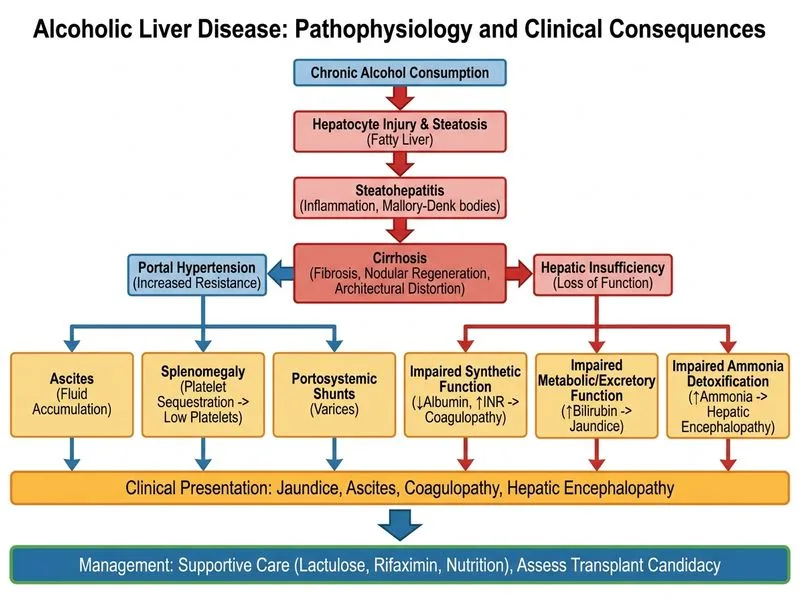
This patient presents with decompensated cirrhosis (ascites, encephalopathy, coagulopathy) secondary to alcoholic liver disease. The AST/ALT ratio >2 and clinical context confirm alcoholic aetiology. The constellation of findings—INR >2.5, bilirubin >5 mg/dL, grade II encephalopathy, and thrombocytopenia—indicates acute-on-chronic liver failure (ACLF) or end-stage cirrhosis.
Management Hierarchy
Key Point
In a patient with decompensated cirrhosis and encephalopathy, immediate priorities are:
Demonstration of 6-month abstinence (or 3 months in selected ACLF cases)
Exclusion of active infection, malignancy, cardiopulmonary contraindications
MELD score calculation and waitlist prioritization
Direct referral without stabilization and abstinence assessment is premature and wastes transplant resources.
Why Not Corticosteroids or Pentoxifylline?
Warning
These agents are indicated only in alcoholic hepatitis (acute inflammation with jaundice, elevated transaminases, and systemic inflammation). This patient has cirrhosis with decompensation, not acute hepatitis. Corticosteroids increase infection risk in cirrhotic patients and are contraindicated in the presence of active encephalopathy or renal dysfunction.
Why Not Ursodeoxycholic Acid?
Ursodeoxycholic acid is used in primary biliary cholangitis (PBC) and primary sclerosing cholangitis (PSC), not alcoholic cirrhosis. It has no proven benefit in alcoholic liver disease.