## Pathophysiology of Portal Hypertension in Alcoholic Cirrhosis **Key Point:** In alcoholic liver disease, portal hypertension develops primarily through **increased intrahepatic vascular resistance** caused by hepatic stellate cell (HSC) activation and fibrosis, not from splenic or hepatic vessel obstruction. ### Mechanism of HSC Activation 1. **Chronic ethanol exposure** → acetaldehyde accumulation and oxidative stress 2. **Hepatocyte injury and apoptosis** → release of damage-associated molecular patterns (DAMPs) 3. **HSC activation** (quiescent → myofibroblast phenotype) 4. **Excessive collagen deposition** → cirrhosis and architectural distortion 5. **Reduced endothelial nitric oxide (NO)** → loss of vasodilatory tone 6. **Increased endothelin-1** → vasoconstriction within sinusoids 7. **Net result:** ↑ intrahepatic resistance → portal hypertension ### Clinical Correlation in This Patient | Finding | Interpretation | |---------|----------------| | AST >> ALT (3.5:1 ratio) | Characteristic of alcoholic hepatitis; AST from mitochondrial damage | | Firm hepatomegaly + ascites | Advanced cirrhosis with portal hypertension | | Spider angiomas + jaundice | Portal hypertension + hepatic synthetic failure | | PT prolongation + low albumin | Hepatic synthetic dysfunction | | Cirrhotic echo pattern + dilated portal vein | Confirmed cirrhosis with hemodynamic compromise | **High-Yield:** The **AST:ALT ratio > 2** in alcoholic liver disease is a classic marker; ALT is relatively spared because ALT is cytoplasmic, whereas AST is mitochondrial and released in alcoholic hepatitis. [cite:Robbins 10e Ch 18] **Clinical Pearl:** Portal hypertension in cirrhosis is **sinusoidal** (intrahepatic) in origin, not extrahepatic. This is why splenectomy does not reverse the hemodynamic abnormality, and why management focuses on reducing intrahepatic resistance (beta-blockers, nitrates) or decompressing the portal system (TIPS, variceal banding). ### Why Stellate Cell Activation Is the Answer HSC activation is the **central event** in fibrogenesis. Activated HSCs: - Produce excessive type I and III collagen - Express α-smooth muscle actin (α-SMA) → contractile phenotype - Release endothelin-1 and other vasoconstrictors - Reduce NO production → loss of sinusoidal vasodilation This creates a **mechanical (fibrosis) + functional (vasoconstriction)** dual increase in resistance. 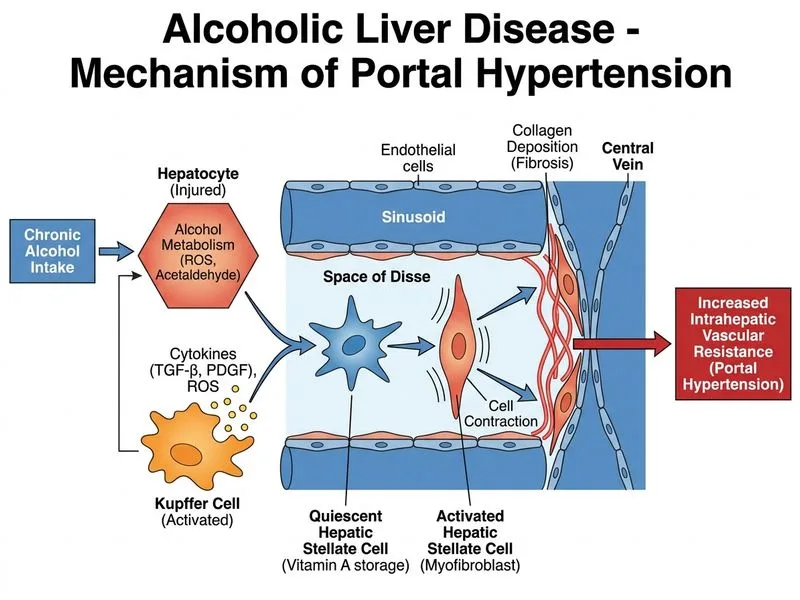
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.