The patient presents with macrocytic anemia (MCV 108 fL) with glossitis, dyspnea, and hypersegmented neutrophils on smear — classic features of megaloblastic anemia. The differential includes vitamin B12 deficiency and folate deficiency.
| Finding | B12 Deficiency | Folate Deficiency |
|---|---|---|
| Serum B12 | Low (<200 pg/mL) | Normal (>200 pg/mL) |
| Serum Folate | Normal or low | Low (<5.4 ng/mL) |
| Neurological signs | Present (paresthesia, ataxia) | Absent |
| Glossitis | Present | Present |
| Source | Pernicious anemia, dietary, post-gastrectomy | Dietary, malabsorption, drugs (MTX, TMP-SMX) |
Harrison 21e Ch 104
Loading illustration…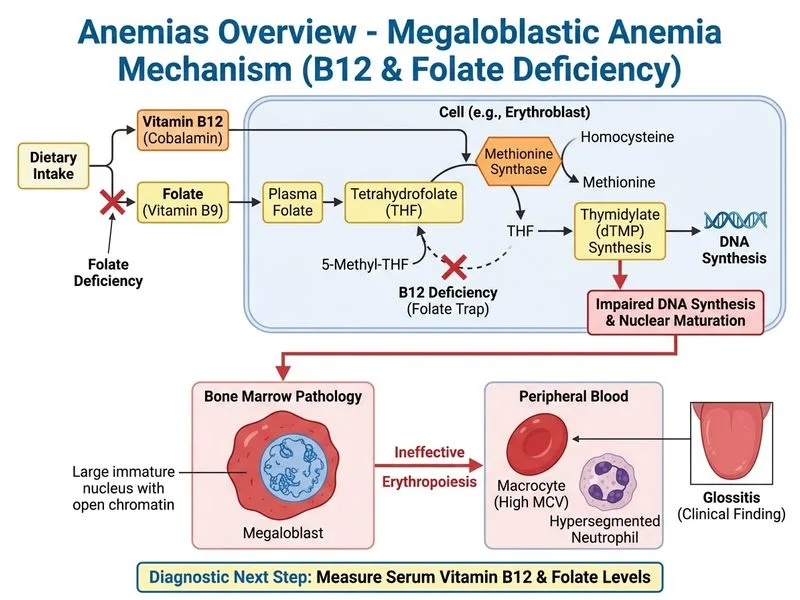
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →