Anemias Overview MCQ — NEET PG Practice Question | NEETPGAI
Anemias Overview
medium
microscope Pathology
A 28-year-old man of Punjabi descent presents to the outpatient clinic with complaints of mild fatigue and jaundice noted incidentally on routine examination. His hemoglobin is 9.8 g/dL, MCV 72 fL, and reticulocyte count is 8% (normal 0.5–2%). Peripheral blood smear reveals target cells, polychromasia, and occasional nucleated RBCs. Serum bilirubin is 3.2 mg/dL (indirect predominant), and haptoglobin is <10 mg/dL. Direct antiglobulin test (DAT/Coombs) is negative. What is the most likely diagnosis?
A. G6PD deficiency with acute hemolysis
B. Hereditary spherocytosis
C. Autoimmune hemolytic anemia
D. Beta-thalassemia trait
Explanation
Diagnostic Approach
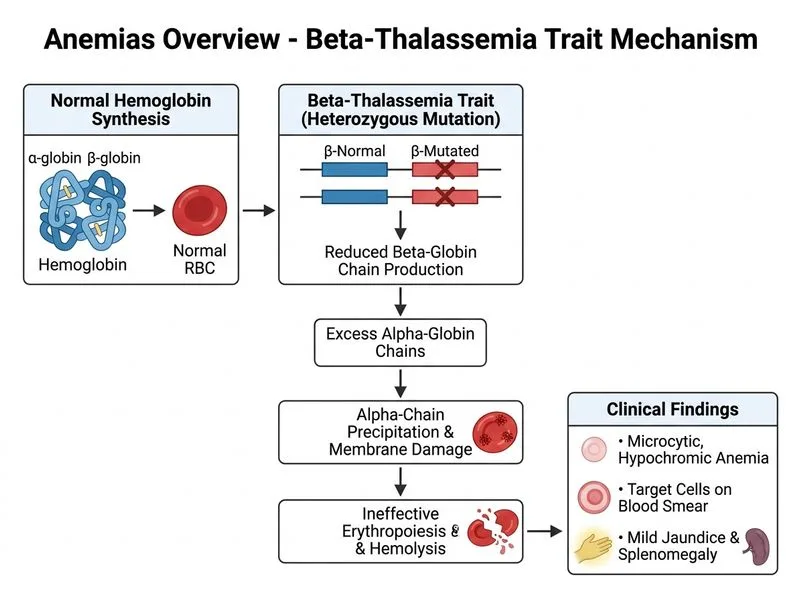
This patient presents with a chronic hemolytic anemia with specific features pointing to beta-thalassemia trait (heterozygous state).
Beta-thalassemia trait (heterozygous) is often asymptomatic or mildly symptomatic and discovered incidentally. The microcytic anemia is disproportionate to the degree of hemolysis.
Differential Diagnosis Table
Table
Feature
β-Thalassemia Trait
Hereditary Spherocytosis
AIHA
G6PD Deficiency
MCV
Micro
Normal/Macro
Normal
Normal
Target cells
Yes
No
No
No
DAT/Coombs
Negative
Negative
Positive
Negative
Haptoglobin
Low
Low
Low
Low
Reticulocyte
Elevated
Elevated
Elevated
Elevated (acute)
Nucleated RBCs
Yes
Rare
Rare
Rare
Osmotic fragility
Normal
Increased
Normal
Normal
Trigger
Chronic
Chronic
Chronic
Oxidative stress
Mnemonic for Thalassemia Trait findings: "MiTT"
Microcytic (MCV <75)
Target cells
Trait (heterozygous, asymptomatic)
Clinical Pearl
In beta-thalassemia trait, the degree of microcytosis is out of proportion to the anemia severity. This is because both hemolysis AND ineffective erythropoiesis contribute to the low MCV.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.