Brachial Plexus MCQ — NEET PG Practice Question | NEETPGAI
Brachial Plexus
medium
bone Anatomy
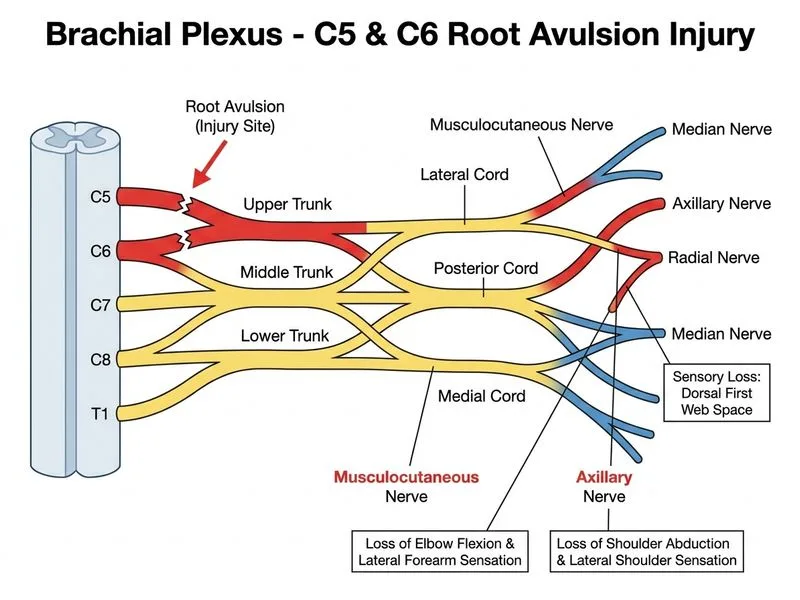
A 28-year-old male motorcyclist is brought to the emergency department following a high-speed collision. On examination, he has a flaccid right arm with loss of sensation over the lateral aspect of the forearm and dorsal first web space. He cannot abduct his shoulder or flex his elbow. There is also loss of sensation over the lateral shoulder. Imaging confirms avulsion of nerve roots from the spinal cord. Which nerve root(s) are most likely avulsed?
A. C5 and C6
B. C6 and C7
C. C7 and C8
D. C8 and T1
Explanation
Clinical Presentation Analysis
The patient presents with a classic upper trunk (Erb's palsy) injury pattern resulting from brachial plexus root avulsion.
Motor Deficits
Loss of shoulder abduction → Supraspinatus and infraspinatus paralysis → Axillary nerve (C5, C6)
Loss of elbow flexion → Biceps and brachialis paralysis → Musculocutaneous nerve (C5, C6)
Dorsal first web space (radial nerve) → C6 dermatome
Lateral shoulder (axillary nerve) → C5 dermatome
Root-Level Anatomy
Table
Nerve Root
Motor Supply
Sensory Supply
Key Reflex
C5
Deltoid, rotator cuff, biceps
Lateral shoulder
Biceps reflex
C6
Biceps, wrist extensors
Lateral forearm, thumb, index
Brachioradialis reflex
C7
Triceps, wrist flexors
Middle finger
Triceps reflex
C8
Intrinsic hand muscles
Medial forearm, ring/little finger
—
T1
Intrinsic hand muscles
Medial arm
—
Key Point
The upper trunk of the brachial plexus is formed by C5 and C6 roots. Avulsion of these roots produces the classic Erb's palsy pattern: "waiter's tip" position (shoulder adducted, internally rotated; elbow extended; forearm pronated).
High-YieldNEET PG
Erb's palsy (upper trunk injury) is the most common brachial plexus injury in birth trauma and traumatic avulsions. Klumpke's palsy (lower trunk, C8–T1) presents with claw hand and medial forearm sensory loss.
Clinical Pearl
The presence of dorsal first web space sensory loss is pathognomonic for C6 involvement—this is the most reliable single sensory marker for upper trunk injury.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.