This patient presents with neurogenic TOS affecting the lower trunk of the brachial plexus bilaterally.
Motor Findings:
Sensory Findings:
Mnemonic: LOAF — Lumbricals (C8–T1), Opponens pollicis (C8–T1), Abductor pollicis brevis (C8–T1), Flexor pollicis brevis (C8–T1) — all supplied by C8–T1 and affected in lower trunk injury.
| Condition | Motor Loss | Sensory Loss | Bilateral? | Cause |
|---|---|---|---|---|
| Lower trunk TOS | Intrinsic hand muscles (C8–T1) | Medial forearm (C8–T1) | Often | Cervical rib, fibrous band |
| Ulnar nerve (cubital tunnel) | Intrinsic hand muscles | Medial 1.5 digits | Rare | Compression at elbow |
| Median nerve (carpal tunnel) | Thenar only | Lateral 3.5 digits | Possible | Compression at wrist |
| Musculocutaneous entrapment | Biceps, brachialis | Lateral forearm | Rare | Compression in arm |
Loading illustration…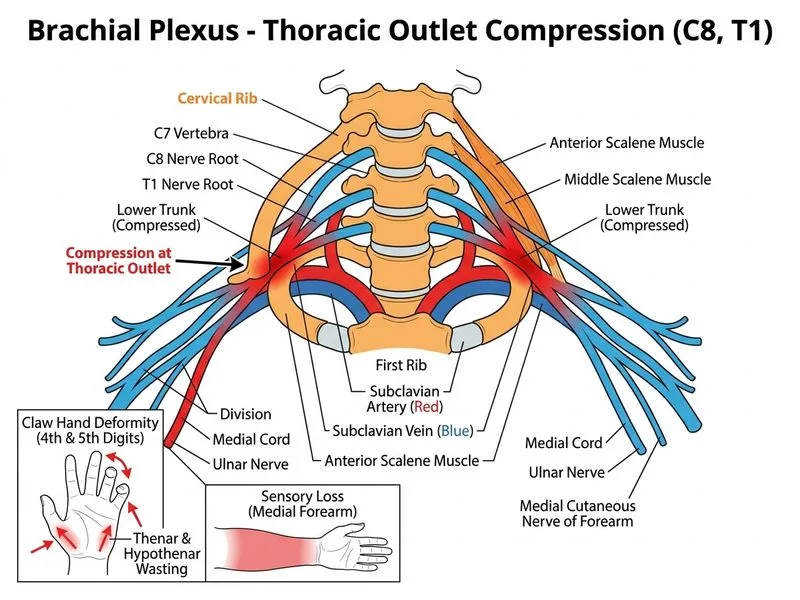
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →