Brachial Plexus MCQ — NEET PG Practice Question | NEETPGAI
Brachial Plexus
medium
bone Anatomy
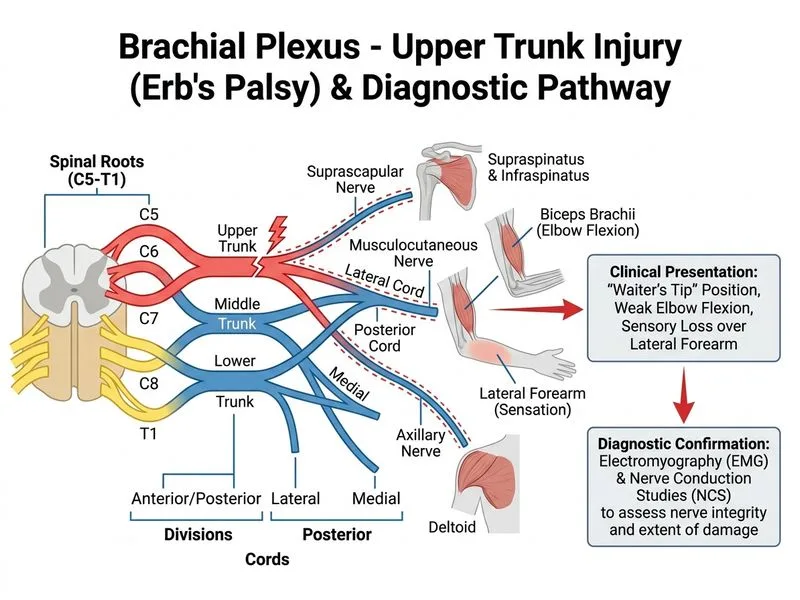
A 28-year-old male presents with loss of sensation over the lateral aspect of the forearm and weakness of elbow flexion following a motorcycle accident with a traction injury to the right upper limb. Clinical examination suggests upper trunk brachial plexus injury. Which investigation is most appropriate to confirm the diagnosis and assess the extent of nerve damage?
A. Electromyography (EMG) and Nerve Conduction Studies (NCS)
B. Computed Tomography (CT) myelography of the cervical spine
C. Magnetic Resonance Imaging (MRI) of the brachial plexus
D. Plain radiograph of the cervical spine and shoulder
Explanation
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Investigation of Choice for Brachial Plexus Injury Assessment
Why EMG/NCS is the Gold Standard
Key Point
EMG and NCS are the most sensitive and specific investigations for confirming brachial plexus injury and determining the extent of nerve damage (axonal loss vs. demyelination).
High-YieldNEET PG
EMG/NCS can:
Detect denervation potentials (fibrillations, positive sharp waves) within 2–3 weeks of injury
Differentiate preganglionic (avulsion) from postganglionic lesions
Assess the severity of injury (Seddon: neurapraxia, axonotmesis, neurotmesis)
Guide prognosis and timing of surgical intervention
Detect subclinical involvement of other nerve roots
Timing and Clinical Utility
Clinical Pearl
EMG is most informative 3–4 weeks post-injury when denervation changes are well-established. Early NCS (within days) can show conduction block in neurapraxia.
It is NOT the first-line confirmatory test because it does not provide functional information about nerve conduction or denervation status, which is essential for prognosis and surgical decision-making.
Comparison of Investigations
Table
Investigation
Sensitivity for Nerve Injury
Functional Assessment
Preganglionic vs. Postganglionic
Timing Post-Injury
EMG/NCS
Very high (>95%)
Excellent
Yes (NCS absent in preganglionic)
3–4 weeks optimal
MRI
Moderate (detects avulsion)
None
Yes (visualizes root avulsion)
Anytime
Plain radiograph
Low (fractures only)
None
No
Anytime
CT myelography
Moderate (CSF leak)
None
Possibly (invasive)
Anytime
Mnemonic
EMG-NCS FIRST — Electromyography and Nerve Conduction Studies provide Functional, Injury-extent, Regeneration-status, and Surgical-timing information.