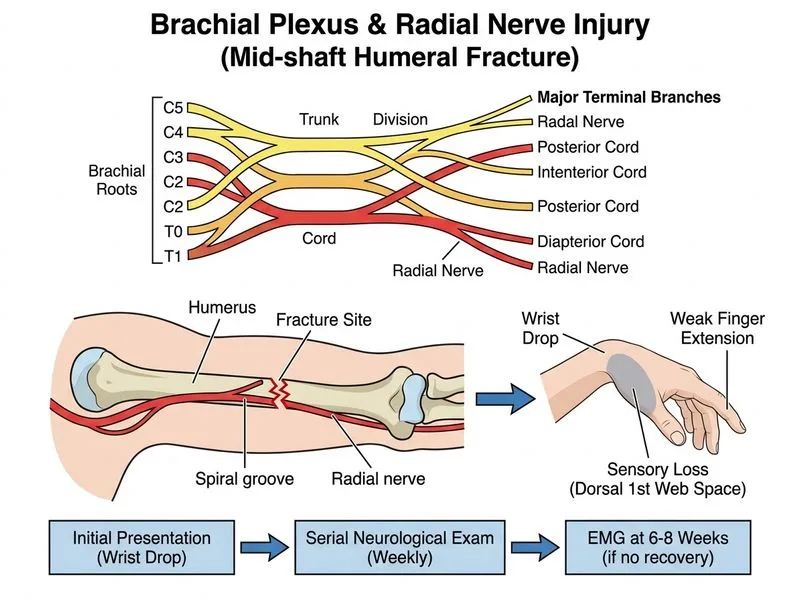
A 35-year-old woman presents with a 2-week history of progressive weakness of wrist and finger extension following a mid-shaft humeral fracture sustained in a fall. Examination reveals wrist drop, weakness of thumb extension, and sensory loss over the dorsal first web space. X-ray confirms a simple mid-shaft fracture with no displacement. What is the most appropriate next step in management?
A. Immediate open reduction and internal fixation with neurolysis
B. Serial neurological examination at weekly intervals and EMG at 6–8 weeks
C. Immediate nerve conduction studies and electromyography
D. Urgent MRI of the arm to rule out nerve transection
Explanation
Clinical Diagnosis
This patient has a radial nerve injury secondary to a mid-shaft humeral fracture. The clinical triad is:
Wrist drop (loss of wrist extension via extensor carpi radialis longus/brevis).
Weakness of thumb extension (extensor pollicis longus).
Sensory loss in the dorsal first web space (radial nerve sensory branch).
Mechanism of Injury
The radial nerve is vulnerable to injury at the mid-shaft of the humerus because it runs in the radial groove on the posterior surface. Fracture fragments or callus formation can compress or stretch the nerve.
Management Strategy
Key Point
Most radial nerve injuries associated with closed humeral fractures are neurapraxia or axonotmesis (not complete transection). These have excellent prognosis for spontaneous recovery over 3–4 months.
High-YieldNEET PG
The correct approach is conservative management with serial neurological assessment:
1.
Serial clinical examination at weekly intervals to document progression or recovery.
2.
EMG/NCS at 6–8 weeks — this is the standard interval to detect denervation changes and confirm the severity of the lesion.
3.
Observation — most radial nerve injuries recover spontaneously within 3–4 months without intervention.
Why Not Immediate Surgery?
Table
Reason
Explanation
Fracture is non-displaced
No indication for ORIF on fracture grounds alone
Nerve injury is likely neurapraxia
Conduction block; spontaneous recovery expected
No clinical signs of transection
Wrist drop and sensory loss are consistent with compression, not division
Early EMG (< 3 weeks) is non-diagnostic
Denervation potentials appear only after 3 weeks
Clinical Pearl
Radial nerve injury at the mid-shaft is the most common nerve injury with humeral fracture and has the best prognosis for spontaneous recovery (>90% recover without surgery). Contrast this with:
Axillary nerve injury (anterior shoulder dislocation) — also usually recovers spontaneously.
Brachial plexus root avulsion — no spontaneous recovery; requires early intervention.
Timeline for Diagnostic and Therapeutic Decisions
Loading diagram...
Mnemonic
RADIAL = Recover After Delayed Interval with Active Limb management — i.e., time and serial exam are the management tools, not immediate surgery.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.