This patient presents with acute decompensated heart failure (HF) with reduced ejection fraction (HFrEF). The dilated left ventricle, low ejection fraction, elevated JVP, and pulmonary edema indicate systolic dysfunction with impaired diastolic function.
In HFrEF:
| Phase | Status in HFrEF | Clinical Outcome |
|---|---|---|
| Isovolumetric contraction | Prolonged but not the primary clinical driver | Reduced stroke volume results, but elevated filling pressures are the main problem |
| Rapid ejection | Severely impaired (low EF = 28%) | Reduced cardiac output, but backward failure (pulmonary edema, JVP elevation) dominates the clinical picture |
| Atrial systole | May be lost if AF develops, but not the primary defect here | Contributes to filling but is not the main cause of the current presentation |
The elevated JVP, pulmonary edema, and S3 gallop all reflect impaired isovolumetric relaxation and abnormal ventricular filling due to increased chamber stiffness and elevated diastolic pressures — not acute loss of contractility during systole.
Loading illustration…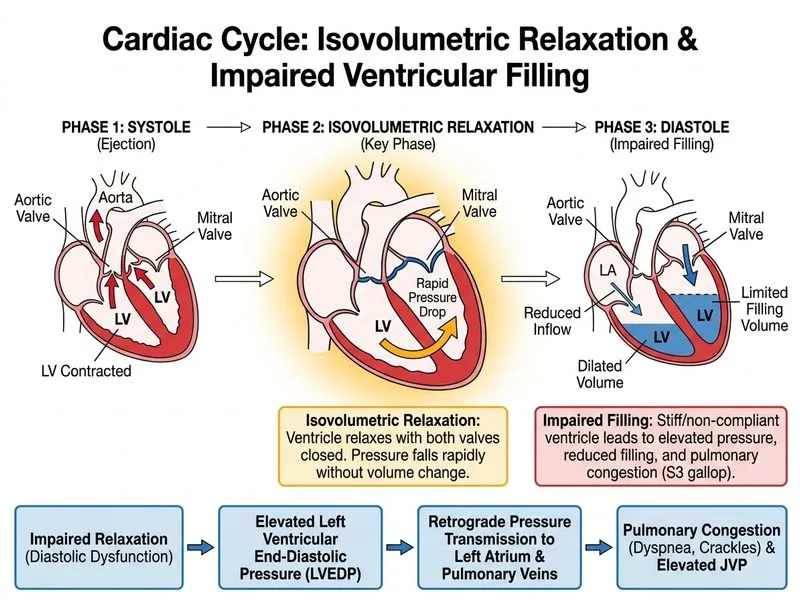
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →