A 38-year-old woman with rheumatic mitral stenosis (mitral valve area 1.2 cm²) presents with progressive dyspnea on exertion and palpitations. On examination, she has an opening snap followed by a low-pitched diastolic murmur at the apex. Her heart rate is 92/min in sinus rhythm. Chest X-ray shows pulmonary congestion. Echocardiography confirms severe mitral stenosis with an ejection fraction of 58%. She has no prior history of atrial fibrillation. What is the most appropriate next step in management?
A. Administer intravenous furosemide and arrange emergency mitral valve replacement
B. Prescribe ACE inhibitors and calcium channel blockers; monitor with serial echocardiography every 6 months
C. Start warfarin anticoagulation immediately and schedule surgical mitral valve replacement
D. Initiate diuretics and beta-blockers to control symptoms; refer for percutaneous mitral balloon valvuloplasty
Explanation
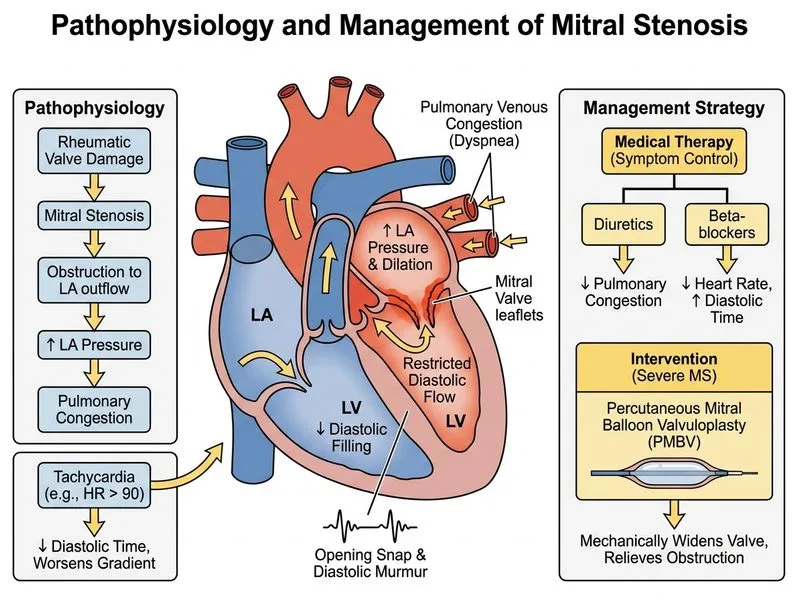
Pathophysiology of Mitral Stenosis and the Cardiac Cycle
Key Point
In mitral stenosis, the narrowed mitral valve orifice obstructs blood flow from the left atrium to the left ventricle during diastole. This increases left atrial pressure, leading to pulmonary venous congestion and eventually pulmonary edema. The left ventricle remains underfilled and has reduced preload, which paradoxically preserves systolic function (EF remains normal or near-normal).
Hemodynamic Consequences
Loading diagram...
Clinical Assessment of This Patient
Table
Feature
Finding
Significance
Mitral valve area
1.2 cm²
Severe stenosis (normal >4 cm²)
Symptoms
Dyspnea on exertion, palpitations
Symptomatic severe MS
Ejection fraction
58%
Preserved (LV not primarily affected)
Rhythm
Sinus rhythm
No atrial fibrillation yet
Chest X-ray
Pulmonary congestion
Elevated LA pressure
Indications for Intervention in Mitral Stenosis
High-YieldNEET PG
Symptomatic patients with severe mitral stenosis (MVA <1.5 cm²) require intervention. The choice between percutaneous mitral balloon valvuloplasty (PMBV) and surgical mitral valve replacement depends on:
1.
Suitability for PMBV: Requires:
No left atrial thrombus (must exclude with TEE)
Favorable valve morphology (Wilkins score <8)
No significant mitral regurgitation
No commissural calcification
2.
This patient is suitable for PMBV because:
Severe symptomatic mitral stenosis
Sinus rhythm (lower thromboembolism risk)
Preserved LV function
No mention of unfavorable morphology
Clinical Pearl
PMBV is the preferred initial intervention in suitable candidates because it:
Avoids surgery and cardiopulmonary bypass
Preserves the native valve
Has good long-term outcomes (70–80% remain symptom-free at 10 years)
Can be repeated if restenosis occurs
Is cost-effective
Medical Management Bridge
While awaiting PMBV:
Diuretics (furosemide): Reduce pulmonary congestion and improve dyspnea
Beta-blockers or rate-limiting calcium channel blockers: Slow ventricular rate, prolong diastole, and allow better LV filling across the stenotic mitral valve
Anticoagulation: Consider if atrial fibrillation develops or if there are other thromboembolic risk factors
Mnemonic: DRAB for Mitral Stenosis Management
Diuretics (reduce congestion)
Rate control (beta-blockers, CCBs)
Anticoagulation (if AF develops)
Balloon valvuloplasty (definitive in suitable cases)
Harrison 21e Ch 291; Robbins 10e Ch 12
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.