Which of the following is the primary mechanism by which cardiac myocytes undergo hypertrophy in response to chronic hypertension?
A. Proliferation of cardiac myocytes through activation of the cell cycle
B. Dedifferentiation of myocytes into progenitor cells
C. Apoptosis of damaged myocytes followed by replacement with new cells
D. Increased protein synthesis and accumulation of contractile proteins without cell division
Explanation
Cardiac Hypertrophy Mechanism
Key Point
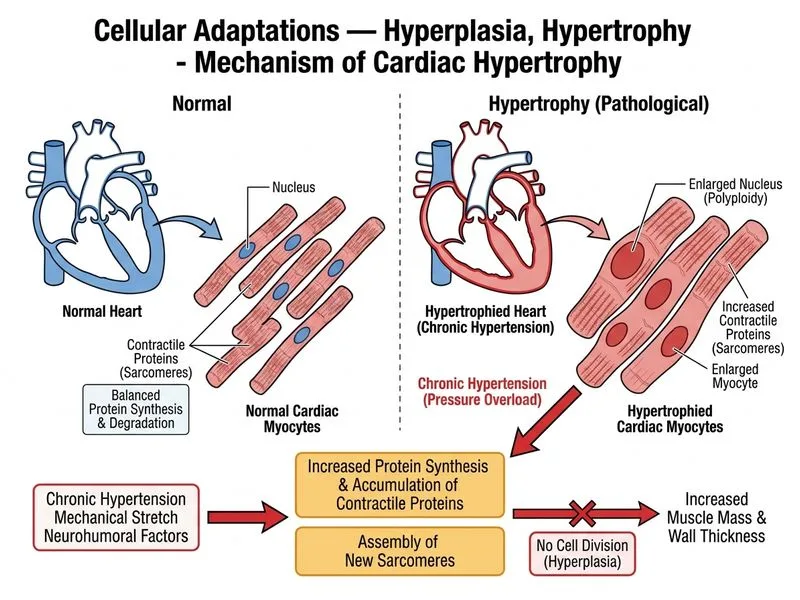
Hypertrophy is defined as an increase in cell size due to increased protein synthesis and accumulation of cellular components, WITHOUT an increase in cell number (no mitosis).
Pathophysiology of Cardiac Hypertrophy
In response to chronic hypertension, cardiac myocytes experience sustained mechanical stress. This triggers:
1.
Activation of growth signaling pathways — mechanical stretch activates receptor tyrosine kinases (RTKs) and G-protein coupled receptors (GPCRs)
2.
Increased protein synthesis — upregulation of mRNA translation and ribosomal activity
3.
Accumulation of contractile proteins — sarcomeric proteins (actin, myosin, tropomyosin) increase in quantity
4.
Cell enlargement — the myocyte increases in volume and mass
5.
NO cell division — cardiac myocytes are terminally differentiated and do not undergo mitosis
Key Distinction: Hypertrophy vs. Hyperplasia
Table
Feature
Hypertrophy
Hyperplasia
Cell size
Increased
Normal or decreased
Cell number
Normal
Increased
Mechanism
Protein synthesis ↑
Cell division ↑
Reversibility
Partially reversible
Reversible
Example
Cardiac hypertrophy in HTN
Endometrial hyperplasia in estrogen excess
High-YieldNEET PG
Cardiac myocytes are post-mitotic cells — they cannot divide. Therefore, the ONLY adaptive response to increased workload is hypertrophy.
Clinical Pearl
Eccentric hypertrophy (chamber dilation + wall thickening) occurs in volume overload; concentric hypertrophy (wall thickening without dilation) occurs in pressure overload like hypertension.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.