A 35-year-old woman with polycystic ovary syndrome (PCOS) presents with endometrial hyperplasia on biopsy due to unopposed estrogen exposure. In contrast, a 28-year-old woman with chronic iron deficiency anemia has compensatory erythroid hyperplasia in her bone marrow. Which finding best distinguishes pathologic endometrial hyperplasia from physiologic erythroid hyperplasia?
A. Reversibility when the causative stimulus is removed
B. Hyperchromatic nuclei and increased mitotic activity
C. Risk of malignant transformation and architectural disorganization
D. Increased number of cells in response to a stimulus
Explanation
Pathologic vs. Physiologic Hyperplasia: The Critical Distinction
Definition and Core Difference
Key Point
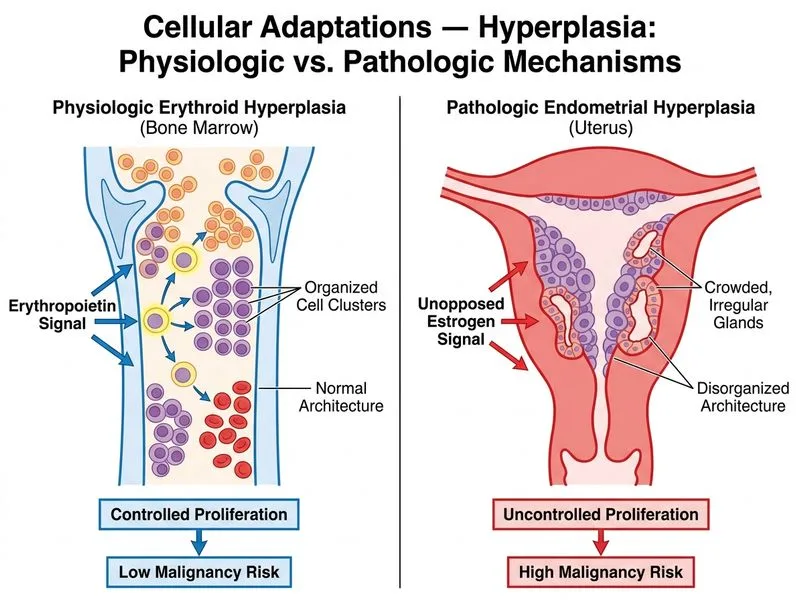
Pathologic hyperplasia (endometrial) carries risk of malignant transformation and shows loss of normal tissue architecture, whereas physiologic hyperplasia (erythroid) is a controlled, reversible response that does not predispose to cancer.
Irreversibility: Atypical changes may persist even after hormone withdrawal
Physiologic Erythroid Hyperplasia
1.
Stimulus: Chronic hypoxia from iron deficiency anemia (adaptive)
2.
Mechanism: Erythropoietin (EPO) stimulates erythroid progenitors proportionally to oxygen demand
3.
Histology: Organized maturation sequence; increased erythroid:myeloid ratio; normal nuclear features
4.
Risk: NO malignant potential
5.
Reversibility: Complete normalization upon iron repletion and hemoglobin restoration
High-YieldNEET PG
The presence of architectural disorganization and malignant potential is the hallmark that separates pathologic from physiologic hyperplasia. Physiologic hyperplasia is always organized, controlled, and reversible.
Mnemonic
PATHOLOGIC = Proliferation with Architectural loss, Transformation risk, Hyperchromatic nuclei, Ounopposed stimulus, Loss of control, Organ dysfunction, Growth beyond need, Irreversible changes, Cancer potential.
Clinical Pearl
Endometrial hyperplasia with atypia is a precancerous lesion requiring treatment (progestin therapy or hysterectomy), whereas erythroid hyperplasia in anemia is a normal compensatory response requiring only iron supplementation. This distinction is critical for clinical management.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.