## CIN-2 Management: Excisional vs Observational Approach **Correct Answer: LEEP with histopathological examination of margins** CIN-2 (cervical intraepithelial neoplasia grade 2) represents a moderate dysplasia with significant risk of progression to invasive cancer if left untreated. The management strategy depends on: ### Key Decision Points: 1. **Biopsy-confirmed CIN-2**: Unlike ASCUS or CIN-1, CIN-2 is NOT managed conservatively 2. **Excisional vs Ablative**: CIN-2 REQUIRES excisional (not ablative) treatment because: - Margins must be assessed histologically - Underlying invasive disease must be excluded - Ablative procedures (laser, cryotherapy) destroy the specimen ### LEEP (Loop Electrosurgical Excision Procedure): - **Gold standard** for CIN-2 management - Provides intact specimen for margin assessment - Allows evaluation for occult invasive disease - Can be both diagnostic and therapeutic - Success rate >95% for CIN-2 when margins are negative ### Follow-up After LEEP: - **Negative margins**: HPV testing or cytology at 6 and 12 months - **Positive margins**: Repeat LEEP or cold knife conization - **Glandular involvement**: Endocervical curettage or cone biopsy **High-Yield**: CIN-2 is the **threshold for mandatory excisional treatment**. CIN-1 may be observed; CIN-3 must be excised. CIN-2 sits at the boundary—biopsy-proven CIN-2 is treated like CIN-3. **Clinical Pearl**: The 2019 ASCCP guidelines emphasize that CIN-2 detected on biopsy warrants excisional treatment, not observation, due to the 30–40% risk of progression to invasive cancer within 5 years if untreated. 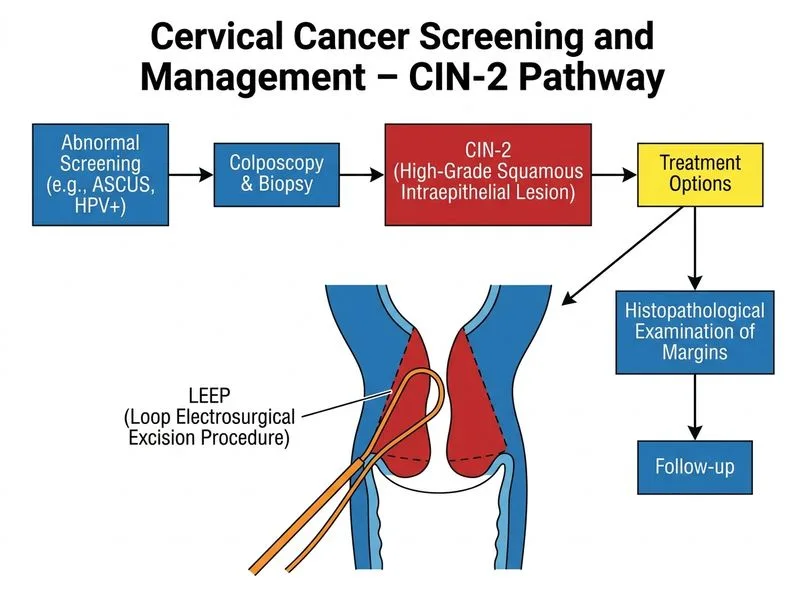
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.