Cholesteatoma MCQ — NEET PG Practice Question | NEETPGAI
Cholesteatoma
medium
ear ENT
A 28-year-old man from rural Rajasthan presents with a 6-month history of foul-smelling otorrhoea from the left ear following a head injury. On otoscopy, there is a perforation in the postero-superior quadrant of the tympanic membrane with granulation tissue visible. Pure tone audiometry shows conductive hearing loss. High-resolution CT temporal bone reveals a soft-tissue density in the epitympanic recess with erosion of the ossicles and lateral semicircular canal. What is the most likely diagnosis?
A. Otosclerosis
B. Cholesteatoma
C. Chronic suppurative otitis media without cholesteatoma
D. Acute suppurative otitis media
Explanation
Clinical Diagnosis: Cholesteatoma
Key Clinical Features in This Case
Key Point
The combination of postero-superior perforation, foul-smelling discharge, ossicular erosion, and lateral semicircular canal erosion on imaging is pathognomonic for cholesteatoma.
Diagnostic Criteria Met
Table
Feature
Finding in Case
Significance
Perforation site
Postero-superior quadrant
Typical location for cholesteatoma (Shrapnell's membrane)
Otorrhoea character
Foul-smelling
Indicates keratinous debris and secondary infection
Imaging findings
Ossicular erosion + SCC erosion
Bone-eroding property of cholesteatoma
Conductive hearing loss
Present
Due to ossicular disruption
Granulation tissue
Visible on otoscopy
Cholesteatoma matrix with inflammatory response
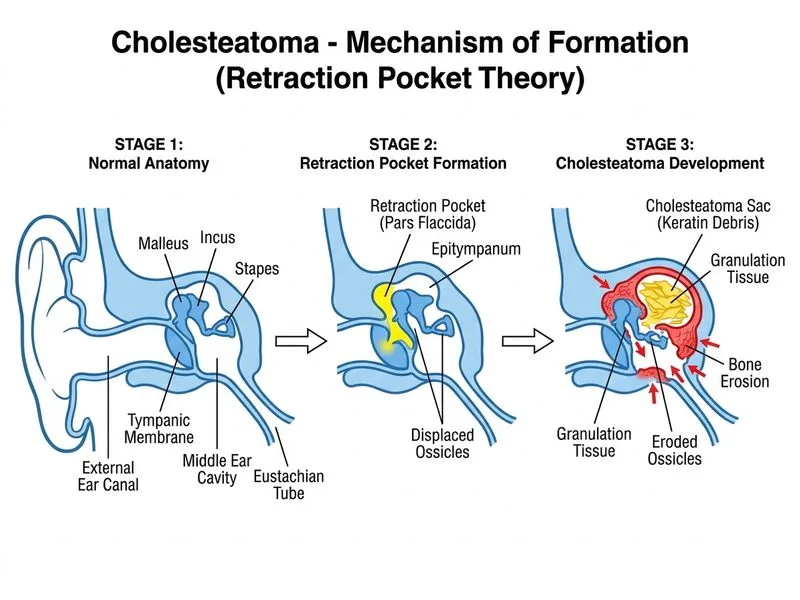
Pathophysiology of Bone Erosion
1.
Pressure necrosis — expanding keratinous mass compresses bone
2.
Enzymatic erosion — collagenase and proteases from inflammatory cells
3.
Osteoclastic activation — bone-resorbing cells recruited by inflammatory mediators
4.
Loss of blood supply — ischemic necrosis of bone
High-Yield: Cholesteatoma vs. CSOM without Cholesteatoma
Table
Feature
Cholesteatoma
CSOM (non-cholesteatoma)
Perforation site
Postero-superior, marginal
Central, safe
Bone erosion
YES (ossicles, SCC, facial canal)
NO
Foul odour
Marked
Mild
Granulation tissue
YES
May be present
CT findings
Soft-tissue density with bone erosion
No bone erosion
Clinical Pearl
Postero-superior perforation with bone erosion on imaging is the single most discriminating feature between cholesteatoma and simple CSOM.
Why Imaging Confirms the Diagnosis
High-YieldNEET PG
HRCT temporal bone is the gold standard for diagnosis and preoperative planning. The presence of:
Soft-tissue density in epitympanic recess
Ossicular erosion (malleus, incus, stapes)
Lateral semicircular canal erosion (risk of vertigo/sensorineural hearing loss)
Possible facial canal dehiscence
All point definitively to cholesteatoma rather than simple CSOM.
Management Implications
Warning
Lateral SCC erosion indicates advanced disease with risk of:
Labyrinthitis ossificans
Sensorineural hearing loss
Vertigo (if labyrinthine fistula develops)
Meningitis (if erosion extends to dura)
Key Point
Surgical intervention (canal wall-up or canal wall-down mastoidectomy) is indicated to prevent intracranial complications.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.