Cholesteatoma MCQ — NEET PG Practice Question | NEETPGAI
Cholesteatoma
medium
ear ENT
A 38-year-old man presents with a 6-month history of foul-smelling otorrhoea and conductive hearing loss. Otoscopy reveals a retraction pocket in the posterosuperior quadrant of the tympanic membrane. Which investigation is most appropriate to confirm the diagnosis of cholesteatoma and assess its extent?
A. Otoacoustic emissions testing
B. Tympanometry
C. Magnetic resonance imaging (MRI) with diffusion-weighted imaging (DWI)
D. High-resolution computed tomography (HRCT) temporal bone
Explanation
Investigation of Choice for Cholesteatoma Diagnosis and Staging
Key Point
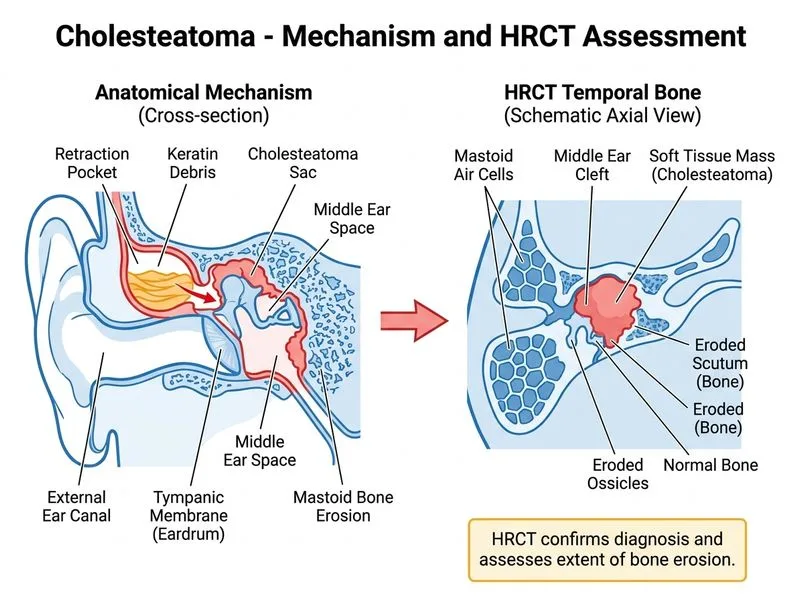
HRCT temporal bone is the first-line investigation for confirming cholesteatoma and assessing its extent, ossicular involvement, and complications prior to surgery.
Why HRCT Temporal Bone is the Correct Answer
1.
Structural/Bony Detail: Provides unparalleled resolution of bony anatomy — demonstrating scutum erosion, ossicular chain destruction, tegmental defects, and labyrinthine involvement.
2.
Preoperative Planning: Mandatory before any tympanomastoid surgery; guides surgical approach and identifies critical anatomical variants (e.g., high jugular bulb, dehiscent facial canal).
3.
Complication Detection: Identifies erosion of the facial canal, lateral semicircular canal, tegmen tympani, and sigmoid plate.
4.
Availability & Cost: Widely available, fast, and far less expensive than MRI — making it the practical first-line choice in most centres.
Why MRI-DWI is NOT the First-Line Investigation
Although MRI with diffusion-weighted imaging (DWI) has very high sensitivity and specificity (~95–100%) for cholesteatoma tissue, it is not the investigation of choice for initial diagnosis because:
It provides poor bony detail — cannot adequately assess ossicular erosion or bony complications.
It is more expensive, less available, and more time-consuming than HRCT.
Its primary role is postoperative surveillance — detecting residual or recurrent cholesteatoma (especially in the context of canal-wall-up mastoidectomy) without exposing the patient to radiation.
Scott-Brown's Otorhinolaryngology and Dhingra's Diseases of Ear, Nose and Throat both designate HRCT temporal bone as the gold-standard preoperative imaging for cholesteatoma.
Clinical Diagnosis vs. Imaging
Clinical Pearl
The diagnosis of cholesteatoma is often made clinically — a retraction pocket in the posterosuperior quadrant (pars flaccida or pars tensa) with foul-smelling otorrhoea is virtually pathognomonic. However, HRCT is mandatory for preoperative planning to define extent, identify complications, and guide surgical strategy. Imaging alone cannot replace clinical assessment.
Cannot reliably differentiate cholesteatoma from granulation tissue on soft-tissue windows alone
MRI DWI
Postoperative surveillance for residual/recurrent disease
Poor bony detail; not first-line for initial diagnosis
Otoacoustic Emissions
Cochlear function screening
Cannot visualize or diagnose cholesteatoma
Tympanometry
Middle ear pressure/compliance assessment
Non-specific; cannot diagnose cholesteatoma
High-YieldNEET PG
The combination of clinical presentation (foul-smelling otorrhoea + posterosuperior retraction pocket) + HRCT findings (scutum erosion, ossicular erosion, soft-tissue mass in epitympanum/mastoid) = definitive workup for cholesteatoma.
Warning
Tympanometry and otoacoustic emissions are functional tests — they cannot diagnose cholesteatoma. MRI-DWI, while highly sensitive, is reserved for detecting residual/recurrent disease postoperatively, not for initial diagnosis.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.