A 38-year-old man from rural India presents with a 6-month history of foul-smelling otorrhoea from the left ear and progressive conductive hearing loss. Otoscopy reveals a retraction pocket in the posterosuperior quadrant with granulation tissue. High-resolution CT temporal bone shows erosion of the scutum and ossicular chain involvement. What is the most appropriate next step in management?
A. Oral antibiotics and topical antifungal agents
B. Surgical exploration with canal wall down (CWD) mastoidectomy
C. Topical antibiotic ear drops and observe for 3 months
D. Audiometry followed by hearing aid fitting
Explanation
Clinical Scenario Analysis
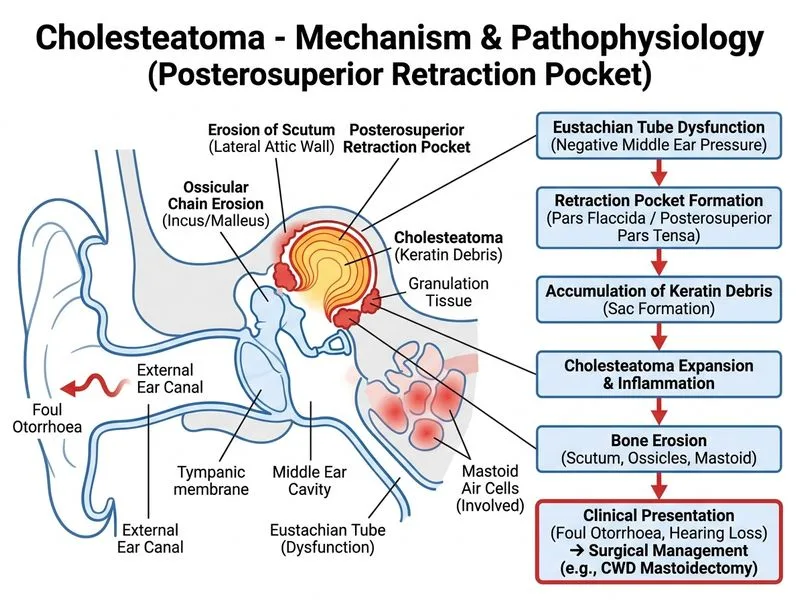
This patient presents with acquired cholesteatoma with imaging evidence of bone erosion and ossicular involvement. The key diagnostic features are:
Retraction pocket in posterosuperior quadrant (classic location)
Foul-smelling discharge (keratinous debris)
CT evidence of scutum erosion and ossicular chain damage
Progressive conductive hearing loss
Management Principles for Cholesteatoma
Key Point
Cholesteatoma is an osteolytic disease that requires surgical intervention. Medical management alone cannot arrest bone erosion or prevent serious complications (facial nerve paralysis, labyrinthitis, meningitis, brain abscess).
High-YieldNEET PG
The two main surgical approaches are:
1.
Canal Wall Down (CWD) — removes disease, exteriorizes mastoid, prevents recurrence (>95%), but creates permanent ear canal abnormality
In this patient, ossicular chain damage means hearing will not be restored even if disease is eradicated. CWD is therefore the definitive, low-recurrence approach and is the standard of care for disease with significant bone erosion.
Mnemonic: CANE — Cholesteatoma with Advanced erosion (ossicles, scutum) → Need External (CWD) approach.
Why Surgery Is Urgent
1.
Risk of facial nerve erosion → paralysis
2.
Risk of labyrinthine fistula → vertigo, sensorineural hearing loss
3.
Risk of intracranial spread → meningitis, abscess
4.
Continued osteolysis → progressive destruction
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.