Cholesteatoma MCQ — NEET PG Practice Question | NEETPGAI
Cholesteatoma
hard
ear ENT
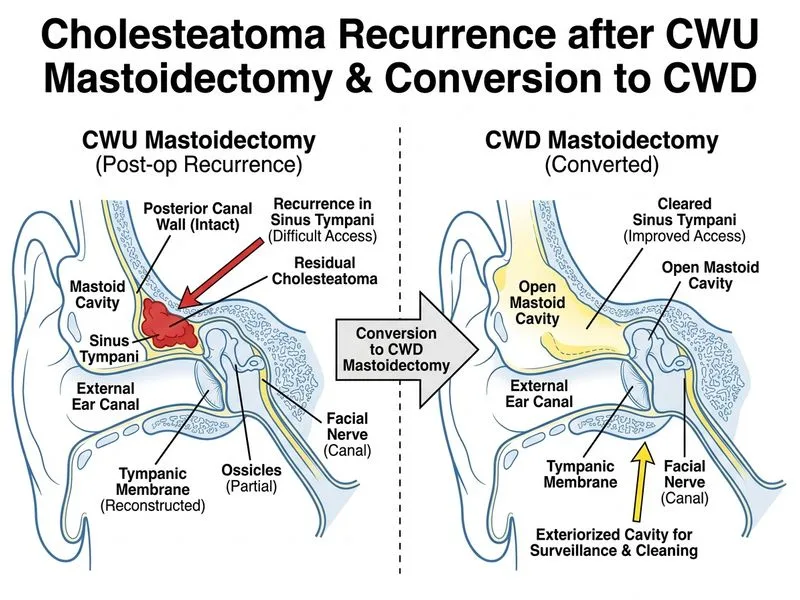
A 28-year-old woman undergoes canal wall up (CWU) mastoidectomy for attic cholesteatoma. At 18 months post-operatively, she presents with recurrent foul-smelling ear discharge and audiometry shows new sensorineural hearing loss in the high frequencies. CT temporal bone shows small residual disease in the sinus tympani. What is the most appropriate next step in management?
A. Conversion to canal wall down (CWD) mastoidectomy
B. Oral antibiotics and topical steroid drops for 8 weeks
C. Repeat CWU surgery with endoscopic-assisted disease removal
D. Observation with 6-monthly audiometry and imaging surveillance
Explanation
Clinical Scenario Analysis
This patient has residual cholesteatoma (disease remaining after initial surgery) with:
Persistent discharge at 18 months post-CWU
New sensorineural hearing loss (high-frequency) — suggests labyrinthine involvement
Imaging confirmation of disease in sinus tympani (notoriously difficult location in CWU approach)
Residual vs Recurrent Disease
Table
Feature
Residual
Recurrent
Timing
Within 6–12 months
>12 months post-op
Cause
Incomplete disease removal at first surgery
Retraction pocket reformation
Incidence after CWU
10–40%
5–15%
Management
Revision surgery (CWD preferred)
CWU revision or CWD
Key Point
Residual disease in sinus tympani is a known failure point of CWU surgery. The sinus tympani is difficult to access via canal wall-preserving techniques and is a common site of disease recurrence.
Why CWD Conversion Is Correct
High-YieldNEET PG
Once residual disease is documented (especially in a difficult location like sinus tympani), the standard of care is conversion to CWD. Reasons:
1.
Sinus tympani is inaccessible via standard CWU approach — even endoscopic assistance has limited efficacy here
2.
New SNHL indicates labyrinthine erosion — risk of further progression
3.
CWD eliminates disease source and prevents recurrence (>95% disease control)
4.
Patient already has canal abnormality risk from first surgery; CWD does not add significant morbidity
Clinical Pearl
The sinus tympani is the "Achilles heel" of CWU surgery — located deep in the anterior epitympanum, it is the most common site of residual disease. Endoscopic-assisted CWU may reduce but does not eliminate this risk.
Mnemonic: SINUS — Sinus tympani Inaccessible → Need Upgrade to Surgical (CWD) approach.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.