| Feature | Congenital Cholesteatoma | Acquired Cholesteatoma |
|---|---|---|
| Tympanic Membrane | Intact | Perforated or retracted |
| Pathogenesis | Embryologic rest of squamous epithelium | Retraction pocket → invagination of epithelium |
| Age at Presentation | Usually <40 years (often childhood/young adult) | Any age; often older children/adults |
| Otorrhea | May be absent initially | Usually present and foul-smelling |
| Location | Anterior to stapes, mesotympanum | Posterosuperior (attic) most common |
| Diagnosis | CT/MRI; intact membrane is key clue | Clinical + imaging |
Congenital cholesteatoma arises from embryologic remnants of squamous epithelium trapped during development (theory of epithelial rest). Acquired cholesteatoma develops secondary to chronic negative middle ear pressure → retraction pocket → epithelial invagination and keratinization. The intact membrane in congenital disease is therefore the single best discriminator.
Loading illustration…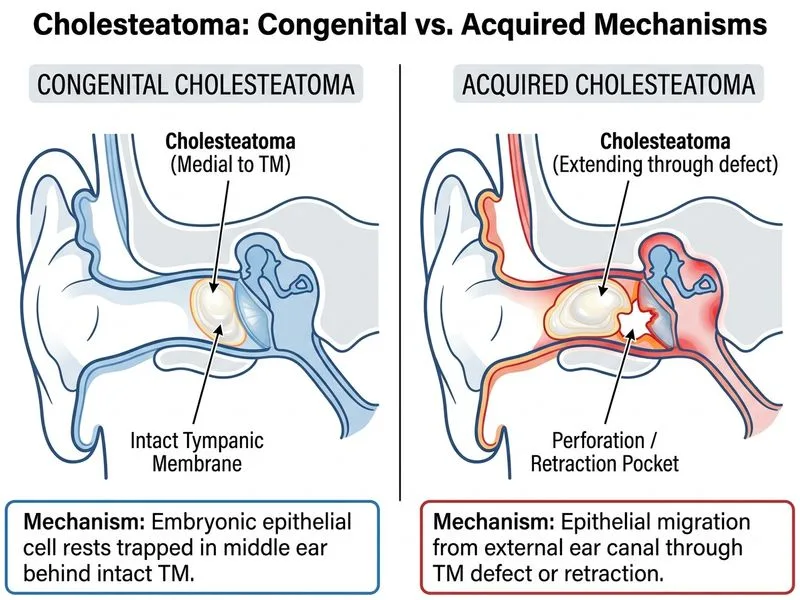
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →