| Investigation | Role | Sensitivity | Timing |
|---|---|---|---|
| Peripheral smear + CBC | Initial screening | Low | Immediate |
| Bone marrow aspirate/biopsy | Morphology assessment | Moderate | Confirmatory |
| BCR-ABL1 (cytogenetics/FISH/RT-PCR) | Definitive diagnosis | >95% | Gold standard |
| Cytochemistry (MPO, PAS) | Lineage confirmation | Moderate | Supportive only |
| Flow cytometry | Rule out blast crisis | Moderate | Staging |
Loading illustration…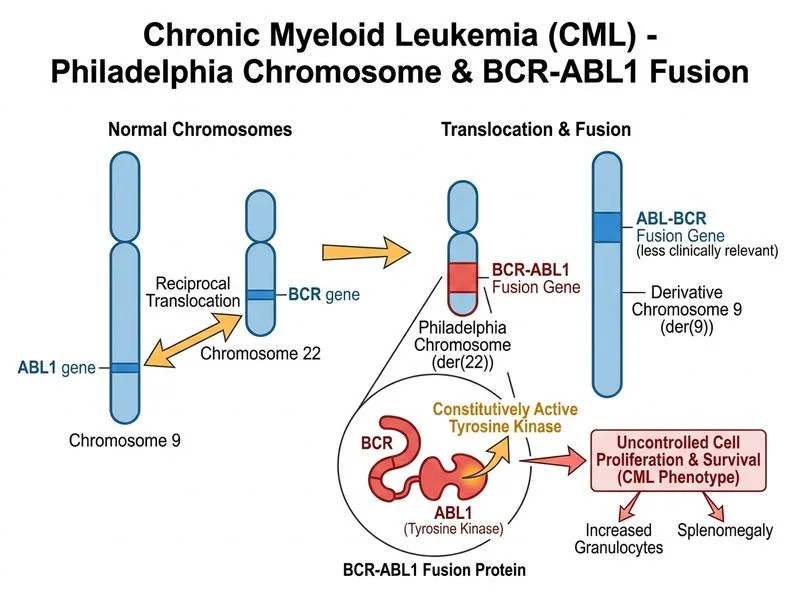
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →