A 28-year-old man from rural Maharashtra presents with a 6-month history of foul-smelling purulent discharge from the left ear following an episode of acute otitis media 8 months ago. He reports conductive hearing loss and occasional ear pain. Otoscopy reveals a large central perforation with granulation tissue and polyps in the external auditory canal. Pure tone audiometry shows air-bone gap of 35 dB. High-resolution CT temporal bone shows erosion of the ossicles and sclerotic mastoid bone. Which of the following is the most appropriate next step in management?
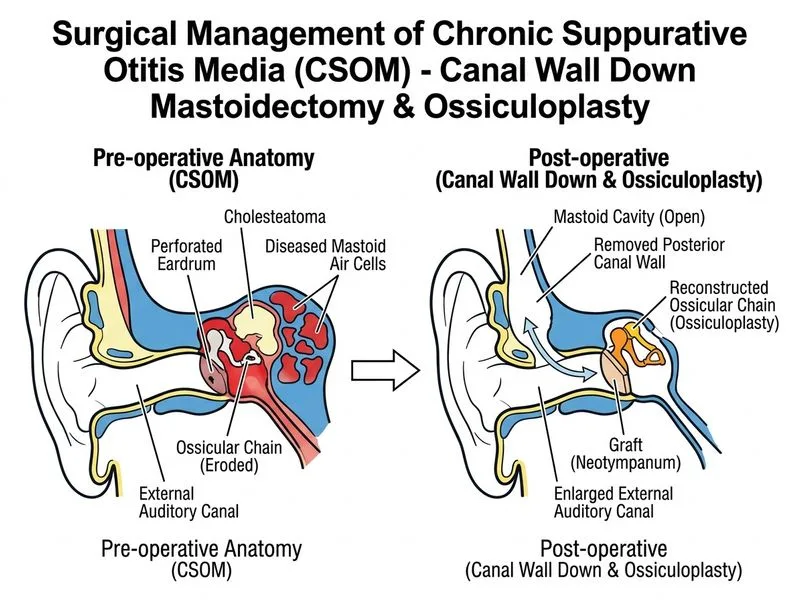
A. Cortical mastoidectomy with canal wall down approach and ossiculoplasty
B. Immediate mastoidectomy with ossiculoplasty
C. Aural toilet and topical antibiotic drops for 4 weeks, then reassess
D. Tympanoplasty alone with canal wall up technique
Explanation
Clinical Assessment
This patient presents with chronic suppurative otitis media (CSOM) with unsafe (atticoantral) disease — evidenced by granulation tissue, polyps, ossicular erosion, and sclerotic mastoid on imaging.
Key Diagnostic Features
High-YieldNEET PG
The presence of granulation tissue and polyps in the canal, combined with ossicular erosion on CT, indicates unsafe CSOM (also called atticoantral disease or cholesteatomatous CSOM).
Key Point
Unsafe CSOM requires surgical intervention — medical management alone is insufficient and carries risk of intracranial complications (meningitis, brain abscess, sigmoid sinus thrombosis).
Ossiculoplasty can be performed in same stage to address conductive loss
Clinical Pearl
In unsafe CSOM with ossicular erosion and sclerotic bone, cortical mastoidectomy with canal wall down offers the lowest recurrence rate (< 5%) and allows staged ossiculoplasty for hearing rehabilitation.
Comparison: CWU vs. CWD
Table
Feature
Canal Wall Up (CWU)
Canal Wall Down (CWD)
Indications
Limited disease, intact canal
Ossicular erosion, extensive disease
Recurrence
10–40% (residual/recurrent)
< 5%
Hearing
Better (ossicular chain preserved)
Permanent CHL (~30 dB)
Complications
Residual disease, repeat surgery
Chronic drainage, water precautions
This case
Not suitable (ossicular erosion)
Indicated
High-YieldNEET PG
Ossicular erosion is a contraindication to CWU — the structural damage cannot be reversed, and CWU leaves residual disease risk.
Why the Correct Answer
Cortical mastoidectomy with canal wall down approach and ossiculoplasty is the gold standard for unsafe CSOM with ossicular erosion because it:
Eradicates disease with minimal recurrence
Allows staged ossiculoplasty for hearing restoration
Addresses both the infection and the conductive loss
Dhingra 8e Ch 16
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.