A 28-year-old woman with a 10-year history of left ear discharge and hearing loss is found on CT temporal bone to have erosion of the stapes footplate and marginal perforation. Otoscopy shows granulation tissue at the perforation margin. She is afebrile with no vertigo. What is the most appropriate next step in management?
A. Oral antibiotics and hearing aid fitting; review in 6 weeks
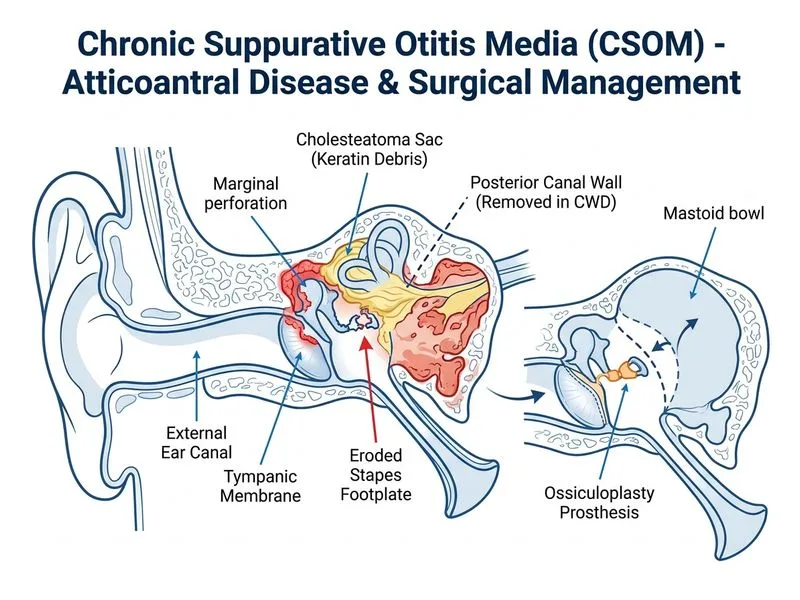
B. Mastoidectomy with canal wall down (CWD) technique and ossiculoplasty
C. Topical antibiotic drops and observation for 3 months before considering surgery
D. Urgent surgical exploration with ossiculoplasty and ossicular chain reconstruction
Explanation
Management of Unsafe CSOM with Ossicular Erosion
Clinical Red Flags Indicating Unsafe CSOM
Key Point
This patient has unsafe CSOM features:
Marginal (attic) perforation — indicates erosion of the posterosuperior canal wall
Granulation tissue — suggests chronic inflammation and bone erosion
Stapes footplate erosion — ossicular involvement with erosion risk
These findings mandate surgical intervention, not conservative management.
Differential: Safe vs. Unsafe CSOM
Table
Feature
Safe CSOM
Unsafe CSOM
Perforation type
Central
Marginal/attic
Ossicular erosion
Absent
Present (stapes, incus, malleus)
Granulation tissue
Absent
Present
Cholesteatoma
Absent
May be present
Management
Conservative first
Surgical
Surgical Decision Tree
Loading diagram...
Why Mastoidectomy with CWD?
High-YieldNEET PG
Marginal perforation with granulation tissue indicates chronic osteitis and risk of recurrent disease. CWD (canal wall down) technique:
1.
Exteriorizes the disease — converts ear canal to mastoid cavity
Allows ossiculoplasty — can reconstruct chain simultaneously
4.
Safe for long-term — low recurrence rate (5–10%) vs. canal wall up (30–40%)
Clinical Pearl
In a patient with marginal perforation and ossicular erosion, CWD is the gold standard because it addresses both the structural defect and the erosive disease process.
Why NOT Conservative Management?
Warning
Conservative management (topical drops, observation) in unsafe CSOM risks:
Progressive ossicular erosion
Sensorineural hearing loss (if stapes footplate erodes further)
Recurrent acute exacerbations
Potential intracranial spread (rare but serious)
Mnemonic: UNSAFE CSOM = SURGERY
Undercut/marginal perforation
Necrosis/granulation tissue
Stapes/ossicular erosion
Attic involvement
Fetid discharge
Expansile lesion risk
Ossiculoplasty Timing
Ossiculoplasty can be performed simultaneously with mastoidectomy in unsafe CSOM because: