This patient presents with severe thrombocytopenia (8,000/µL) with a long history of easy bruising and mucocutaneous bleeding, but normal coagulation studies (PT, aPTT) and a normocellular bone marrow with adequate megakaryocytes. These findings are pathognomonic for Immune Thrombocytopenia (ITP).
| Feature | ITP | TTP | DIC | HUS |
|---|---|---|---|---|
| Platelet count | <30,000/µL | <30,000/µL | <100,000/µL | <30,000/µL |
| PT/aPTT | Normal | Normal | Prolonged | Normal |
| Fibrinogen | Normal | Normal | ↓ | Normal |
| Schistocytes | Absent | Present | Present | Present |
| Renal involvement | Absent | Present (MAHA) | Present | Present (HUS hallmark) |
| Neurological signs | Absent | Present (TTP hallmark) | Absent | Absent |
| BM megakaryocytes | Adequate/↑ | Normal | Normal/↓ | Normal |
"ITP = Isolated Thrombocytopenia with Preserved coagulation" — when you see low platelets + normal PT/aPTT + normal fibrinogen + adequate BM megakaryocytes, think ITP first.
Bleeding time is prolonged in ITP because platelet count is so low that platelet plug formation is impaired, even though individual platelet function is normal. Modern labs have abandoned bleeding time; diagnosis is clinical + platelet count + BM exam.
Robbins 10e Ch 13
Loading illustration…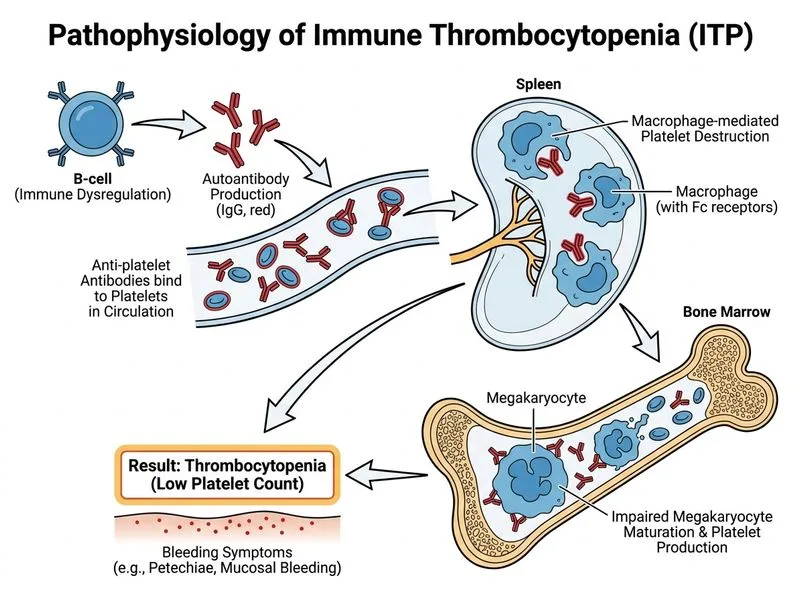
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →