This patient has cirrhosis-induced coagulopathy, a complex disorder combining:
| Feature | Cirrhosis | DIC |
|---|---|---|
| Fibrinogen | Low (chronic) | Very low (acute consumption) |
| Platelets | Low (splenomegaly) | Very low (consumption) |
| PT/aPTT | Prolonged (factor deficiency) | Prolonged (consumption) |
| D-dimer | Mildly ↑ (impaired clearance) | Markedly ↑ (active thrombin generation) |
| Response to FFP | Poor/transient | Good initial response |
| Vitamin K response | Poor (liver cannot use it) | Good (if deficiency component) |
| Antithrombin III | Normal/high | Low (consumed) |
| Prothrombin time trend | Chronic, stable or worsening | Acute, rapidly worsening |
Ongoing consumption (Option A): While some consumption may occur during active bleeding, the failure of FFP to sustain PT correction is not typical of DIC. In DIC, FFP transfusion usually produces at least a transient improvement because factors are being actively consumed and replaced. Here, the PT remains persistently prolonged despite FFP, indicating the problem is production failure, not consumption.
Vitamin K deficiency alone (Option C): Cirrhotic patients often have vitamin K deficiency (malabsorption, antibiotic use), but vitamin K alone cannot correct the coagulopathy because the liver cannot activate the vitamin K-dependent factors. FFP + vitamin K should improve PT in pure vitamin K deficiency; failure to do so indicates hepatic dysfunction.
Platelet dysfunction (Option D): While cirrhotic patients may have qualitative platelet dysfunction, the prolonged PT is a coagulation cascade abnormality, not a platelet function problem. Platelet dysfunction would cause prolonged bleeding time (now abandoned) or platelet aggregation defects, not prolonged PT.
"Cirrhosis = production failure; DIC = consumption failure." FFP works in DIC (replaces consumed factors) but fails in cirrhosis (liver cannot make new factors). Vitamin K works in vitamin K deficiency but fails in cirrhosis (liver cannot use it).
Harrison 21e Ch 297
Loading illustration…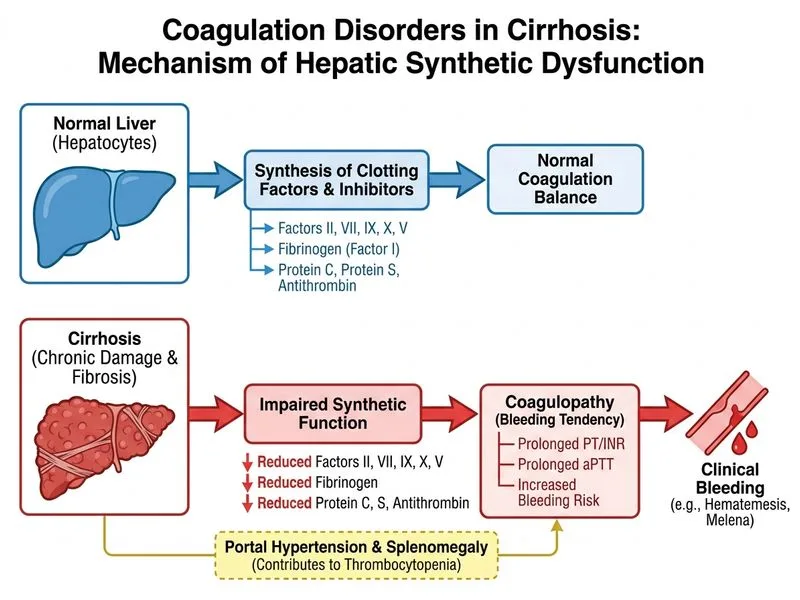
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →