Which of the following is the most common early systemic complication of long bone fractures?
A. Fat embolism syndrome
B. Acute respiratory distress syndrome
C. Disseminated intravascular coagulation
D. Pulmonary thromboembolism
Explanation
Early Systemic Complications of Long Bone Fractures
Key Point
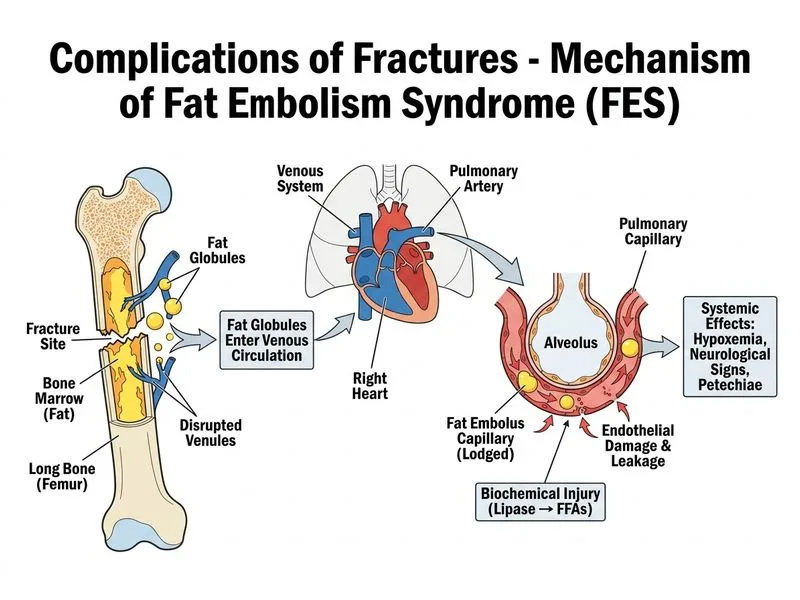
Fat embolism syndrome (FES) is the most common early systemic complication, occurring within 24–72 hours of long bone fracture, particularly femur, tibia, and pelvis.
Pathophysiology
Fat embolism occurs when marrow fat enters the venous circulation through:
1.
Disrupted medullary vessels at fracture site
2.
Increased intramedullary pressure forcing fat globules into systemic circulation
3.
Mechanical obstruction and chemical injury to pulmonary capillaries