Complications of Fractures MCQ — NEET PG Practice Question | NEETPGAI
Complications of Fractures
medium
bone Orthopedics
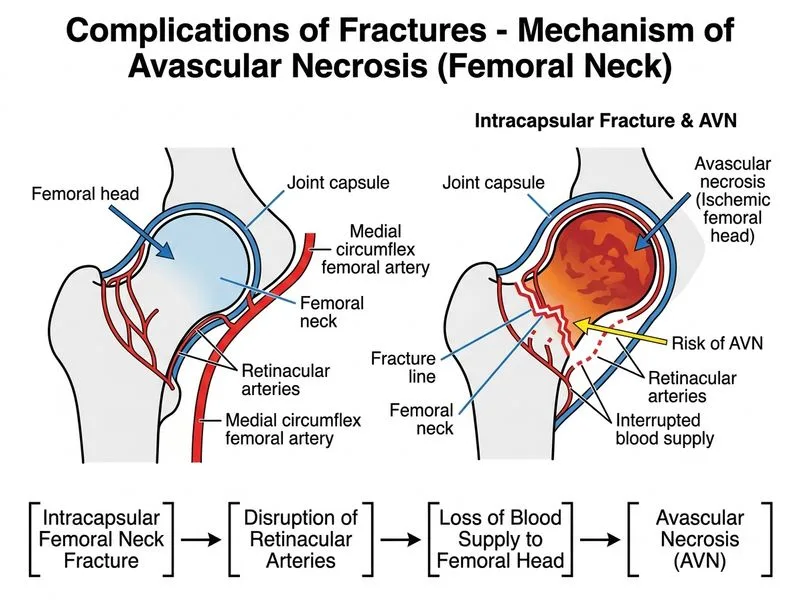
Avascular necrosis (AVN) is most likely to occur following fracture of which bone?
A. Femoral neck (intracapsular fracture)
B. Distal radius
C. Proximal humerus
D. Proximal tibia
Explanation
Avascular Necrosis: Fracture-Related Risk
Key Point
Femoral neck fractures, particularly intracapsular (subcapital and transcervical), carry the highest risk of AVN due to the precarious blood supply to the femoral head.
Femoral head becomes dependent on retrograde flow via ligamentum teres (minimal in adults)
3.
Prolonged ischemia → osteocyte death → collapse of articular surface
4.
Typically manifests 6–24 months post-fracture
Mnemonic
SHAFT — Sites of high AVN risk:
Scapula (proximal pole)
Humerus (proximal)
Astragalus (talus)
Femoral head (femoral neck fracture)
Talus
Clinical Pearl
Early diagnosis of AVN requires high clinical suspicion. MRI is the gold standard for detecting AVN before radiographic changes appear (T1-weighted images show band-like low signal).
Prevention & Management
Early reduction: < 12 hours (reduces ischemic time)
Internal fixation: cannulated screws or plates to maintain reduction
Monitoring: serial radiographs at 6, 12, 18 months; MRI if symptoms develop
Treatment of established AVN: core decompression (early stage), arthroplasty (advanced stage)
Rockwood & Green's Fractures in Adults Ch 51
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.