This patient has a closed fracture (no break in skin at time of injury) with signs of infection appearing 3 days post-injury. The combination of:
...points to Fracture-Related Infection (FRI) — also termed post-traumatic osteomyelitis in traditional Indian curricula (Maheshwari's Essential Orthopaedics) — rather than hematogenous osteomyelitis or cellulitis.
| Option | Reason Excluded |
|---|---|
| A — Hematogenous osteomyelitis | Requires a distant bacteremia source (e.g., skin infection, UTI, endocarditis) or immunosuppression — none mentioned. Typically affects metaphysis of long bones in children without preceding fracture. |
| B — Fat embolism syndrome | Presents 24–72 h post-fracture with respiratory distress, petechiae, and confusion (Gurd's criteria) — not with localized bone infection signs or radiological lucencies. |
| D — Cellulitis | Soft-tissue infection only; does not produce periosteal reaction or cortical lucencies on plain radiograph. Systemic markers are usually milder, and there is no bone involvement. |
Clinical Pearl (Harrison's / Maheshwari): Early recognition and aggressive surgical debridement (removal of devitalized bone and soft tissue) combined with prolonged antibiotics (4–6 weeks IV, then oral) are essential to prevent progression to chronic osteomyelitis and non-union — the two most feared complications.
High-Yield for NEET PG: In a closed fracture with early fever, local bone signs, and radiological changes — the answer is FRI / post-traumatic osteomyelitis (Option C). Hematogenous osteomyelitis requires a bacteremia source; cellulitis lacks bone radiological changes.
Loading illustration…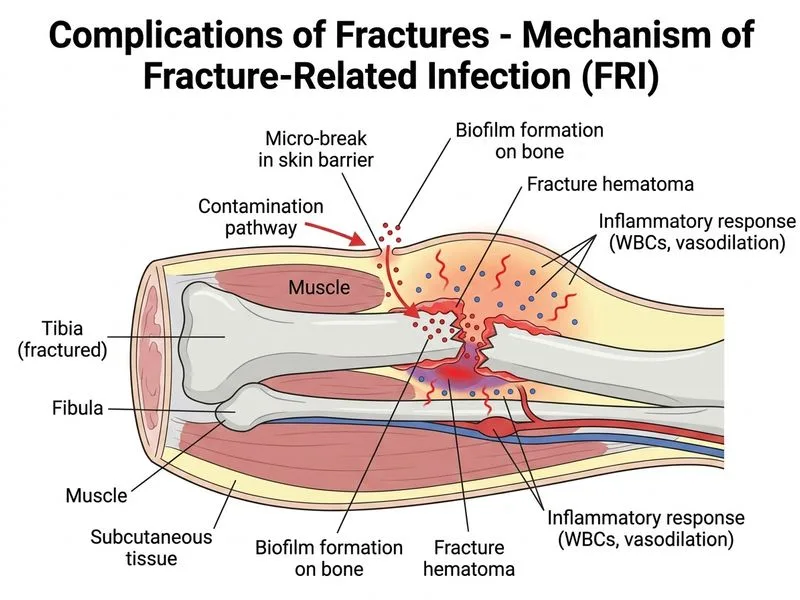
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →