Complications of Fractures MCQ — NEET PG Practice Question | NEETPGAI
Complications of Fractures
medium
bone Orthopedics
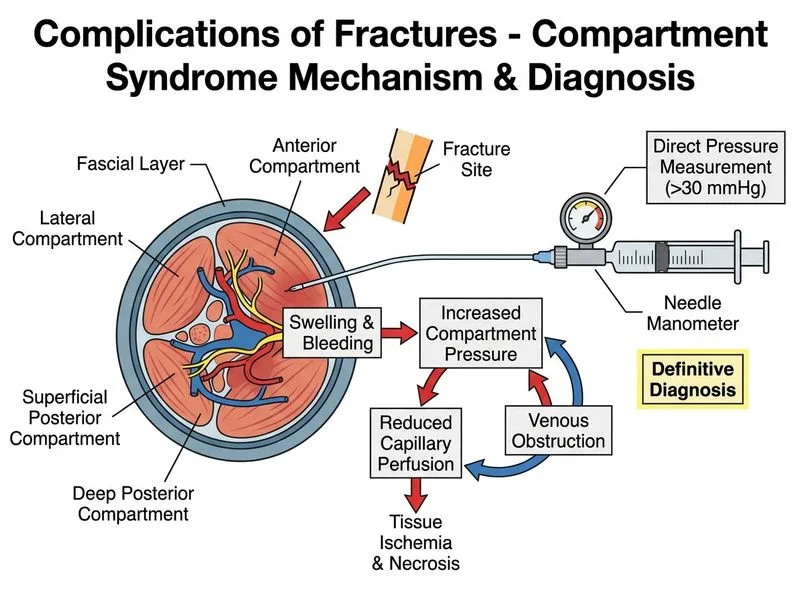
A 32-year-old male presents with a closed fracture of the femoral shaft sustained 8 hours ago. On examination, the limb is swollen and tense. You suspect compartment syndrome. Which investigation is most sensitive and specific for confirming compartment syndrome?
A. Doppler ultrasound of the femoral artery
B. Plain radiograph of the femur
C. Compartment pressure measurement using a needle manometer
D. MRI of the thigh
Explanation
Diagnosis of Compartment Syndrome
Key Point
Compartment syndrome is a surgical emergency requiring early diagnosis based on clinical suspicion and objective pressure measurement — not imaging.
Why Compartment Pressure Measurement is Gold Standard
Compartment syndrome results from increased interstitial pressure within a fascial compartment, compromising microvascular perfusion and tissue viability. The diagnosis rests on:
1.
Clinical suspicion (pain out of proportion, pain on passive stretch, paresthesias, pallor, pulselessness is a late sign)
2.
Objective pressure confirmation using a needle manometer or slit catheter inserted into the compartment
High-YieldNEET PG
The critical pressure threshold is when compartment pressure exceeds diastolic blood pressure by >30 mmHg (or absolute pressure >30 mmHg in normotensive patients). This is the indication for emergency fasciotomy.
Why Other Investigations Fail
Table
Investigation
Limitation
Plain radiograph
Shows only bone; cannot assess soft tissue pressure or muscle viability
Doppler ultrasound
Assesses vascular flow but does not measure compartment pressure; pulses may remain intact early in CS
MRI
Slow, not available emergently; delays definitive treatment
Clinical Pearl
Compartment syndrome is a clinical diagnosis confirmed by pressure measurement. Do NOT wait for imaging. Delay in fasciotomy beyond 6–8 hours leads to irreversible muscle necrosis and permanent disability.
Warning
Absence of pulselessness does NOT rule out compartment syndrome — it is a late finding. Proceed to fasciotomy based on clinical suspicion + pressure confirmation.
Mnemonic
5 P's of compartment syndrome — Pain (out of proportion), Pressure (elevated compartment pressure), Paresthesias, Pallor, Pulselessness (late). The first three are early; the last two are late.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.