Consolidation vs Collapse on Chest X-ray MCQ — NEET PG Practice Question | NEETPGAI
Consolidation vs Collapse on Chest X-ray
hard
scan Radiology
A 72-year-old man with lung cancer presents with progressive dyspnea over 3 days. Chest X-ray shows opacification of the entire right hemithorax with rightward tracheal deviation and elevation of the right hemidiaphragm. The left lung is hyperinflated. What is the most appropriate next step in management?
A. Arrange urgent flexible bronchoscopy to assess airway patency and relieve obstruction
B. Perform rigid bronchoscopy with therapeutic aspiration of mucus plug
C. Obtain a CT chest to assess tumour burden and plan intervention
D. Start empirical antibiotics for presumed pneumonia
Explanation
Clinical Diagnosis
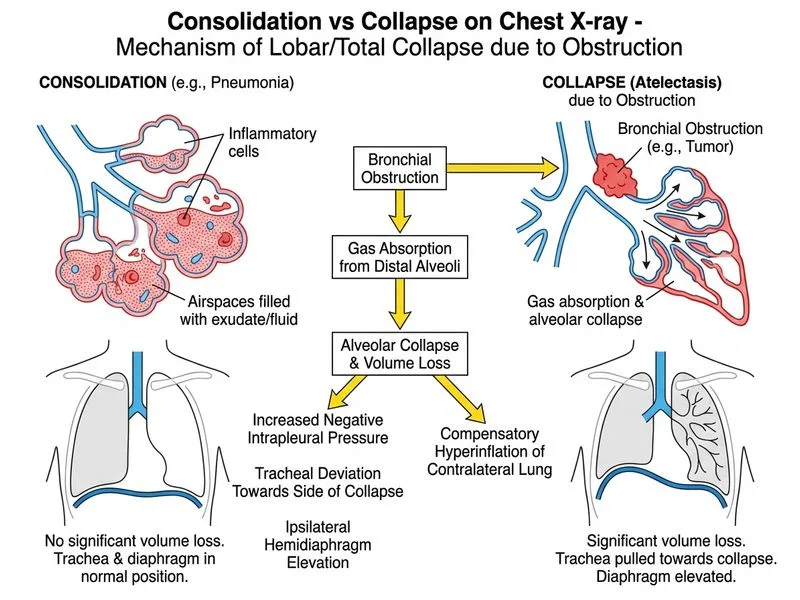
The radiological findings are diagnostic of whole-lung collapse, not consolidation:
Rightward tracheal deviation (shift toward affected side = volume loss)
Elevation of right hemidiaphragm (volume loss sign)
Hyperinflation of contralateral lung (compensatory)
Opacification with ipsilateral mediastinal shift = collapse, not consolidation (consolidation causes no shift or contralateral shift if massive)
Key Point
In a lung cancer patient with acute whole-lung collapse, the most likely cause is endobronchial obstruction — tumour, mucus plug, or blood clot occluding the right main bronchus.
Consolidation vs Collapse: Radiological Differentiation
Table
Feature
Consolidation
Collapse
Tracheal position
Midline or away
Shifts toward affected side
Hemidiaphragm
Normal position
Elevated
Contralateral lung
Normal
Hyperinflated (compensatory)
Mediastinal shift
None / contralateral
Ipsilateral
Urgent intervention
Antibiotics, supportive
Airway clearance, bronchoscopy
Why Flexible Bronchoscopy is the Best Next Step
High-YieldNEET PG
In a lung cancer patient with acute collapse and progressive dyspnea:
1.
Flexible bronchoscopy is the first-line diagnostic AND therapeutic tool for endobronchial obstruction
2.
Allows direct visualization of the right main bronchus
3.
Can remove obstructing tumour, mucus plug, or blood clot under direct vision
4.
Restores ventilation acutely and provides tissue diagnosis if needed
5.
Widely available, can be performed at bedside or in endoscopy suite with sedation
Why not the other options?
Option A (Empirical antibiotics): The ipsilateral tracheal shift confirms collapse, not consolidation/pneumonia. Antibiotics alone will not relieve mechanical obstruction.
Option B (Rigid bronchoscopy): Rigid bronchoscopy has a role in massive haemoptysis or when large rigid instrumentation is required (e.g., stenting, laser debulking of bulky tumour). However, it requires general anaesthesia and is not the first step — flexible bronchoscopy is performed first to assess the airway and attempt therapeutic aspiration. Rigid bronchoscopy is escalated if flexible bronchoscopy is insufficient.
Option C (CT chest): While CT provides valuable staging and anatomical information, it delays urgent intervention in a patient with progressive dyspnea from acute collapse. Bronchoscopy is both diagnostic and immediately therapeutic.
Clinical Pearl (Harrison's Principles, 21st ed.): Flexible bronchoscopy is the preferred initial approach for endobronchial obstruction in malignancy. Rigid bronchoscopy is complementary and reserved for cases requiring mechanical debulking, stent placement, or when flexible bronchoscopy fails to relieve obstruction. The SME note correctly highlights that both modalities have roles — but flexible bronchoscopy is the most appropriate next step given its availability, safety profile, and dual diagnostic-therapeutic utility.
Mnemonic
COLLAPSE = Cough, Loss of volume, Lateral (ipsilateral) shift, Apex elevated, Pneumonia unlikely, Silhouetting variable, Endobronchial obstruction — think airway obstruction first in malignancy.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.