Corneal Ulcer — Bacterial and Fungal MCQ — NEET PG Practice Question | NEETPGAI
Corneal Ulcer — Bacterial and Fungal
medium
eye Ophthalmology
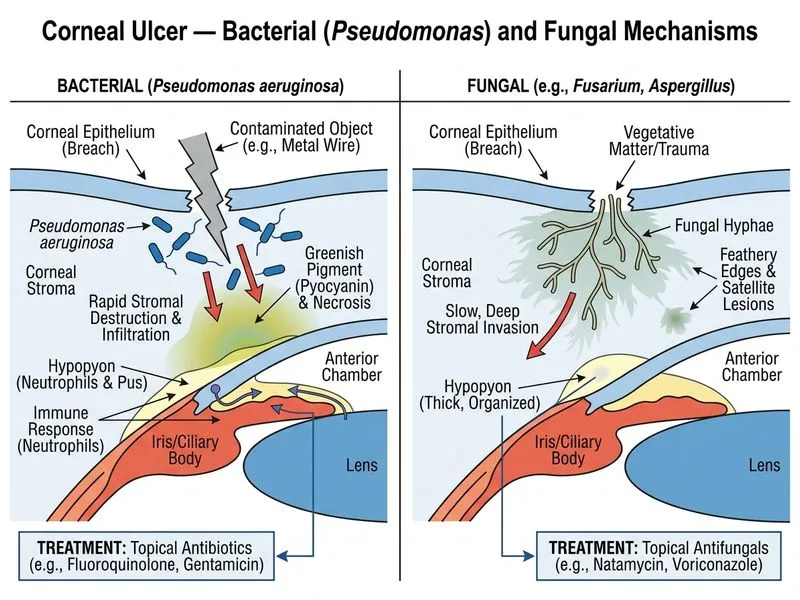
A 38-year-old male labourer from Tamil Nadu presents with a 3-day history of severe left eye pain, purulent discharge, and blurred vision following a minor corneal abrasion from a contaminated metal wire. On examination, visual acuity is 6/36. Slit-lamp shows a 3 mm central corneal ulcer with a greenish tinge, stromal infiltration, and a 2 mm hypopyon. Gram stain of corneal scrapings shows Gram-negative rods. Culture on MacConkey agar grows a mucoid, non-lactose-fermenting colony. What is the most likely organism and the preferred topical antibiotic?
A. *Pseudomonas aeruginosa*; topical gentamicin 0.3% or fluoroquinolone
B. *Neisseria gonorrhoeae*; topical ceftriaxone 1% or tetracycline
C. *Klebsiella pneumoniae*; topical amoxicillin-clavulanate or cephalosporin
D. *Vibrio cholerae*; topical chloramphenicol 0.5% or aminoglycoside
Explanation
Organism Identification
Key Point
The combination of:
Gram-negative rod
Mucoid, non-lactose-fermenting colony on MacConkey agar
Greenish tinge to the ulcer
Rapid progression (3 days) with stromal infiltration and hypopyon
...is pathognomonic for _Pseudomonas aeruginosa_, the most common Gram-negative cause of bacterial corneal ulcer in India.
High-YieldNEET PG
Pseudomonas characteristics:
Aerobic, motile, Gram-negative rod
Produces pyoverdine (greenish pigment) and pyocyanin (blue pigment)
Non-lactose-fermenting on MacConkey (appears as clear/colorless colonies)
Mucoid phenotype indicates biofilm production (virulence factor)
Produces proteolytic enzymes → rapid stromal melting and perforation risk
Differential Diagnosis of Gram-Negative Corneal Ulcers
Topical gentamicin (aminoglycoside) or fluoroquinolone (e.g., ofloxacin, moxifloxacin) are the preferred agents for Pseudomonas corneal ulcer because:
1.
High corneal penetration and bactericidal activity
2.
Broad spectrum covers other Gram-negative and Gram-positive organisms
3.
Fluoroquinolones have superior corneal bioavailability
Clinical Pearl
Pseudomonas is an obligate aerobe and produces proteolytic enzymes that can cause rapid stromal melting and perforation within 24–48 hours. Aggressive topical therapy (hourly instillation) and close monitoring are essential. Systemic fluoroquinolone (e.g., ciprofloxacin 500 mg BD) should be added for severe cases.
Warning
Avoid topical steroids in Pseudomonas ulcer — they accelerate stromal melting and perforation. Do NOT use topical penicillins or cephalosporins alone; aminoglycosides or fluoroquinolones are superior.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.