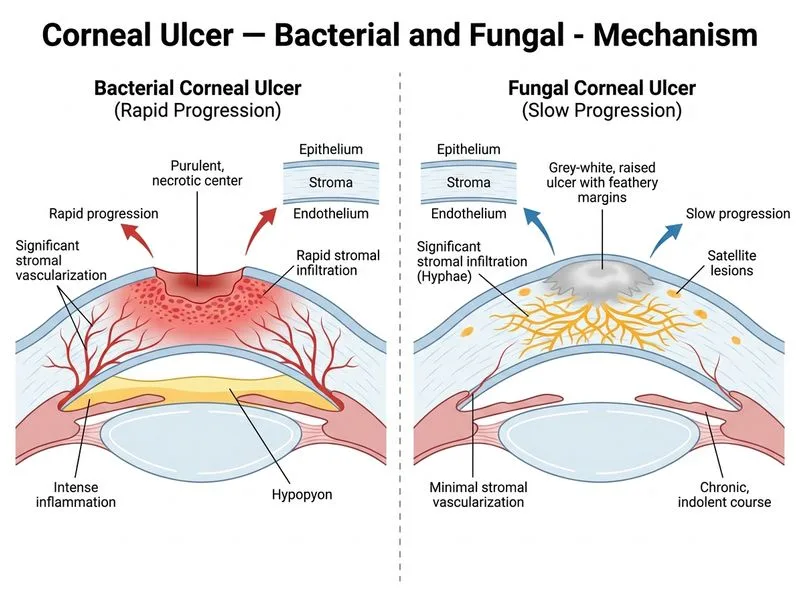
A 52-year-old farmer from rural Maharashtra presents with corneal ulcer following a thorn prick injury 10 days ago. On slit-lamp examination, the ulcer has a grey-white, raised, indurated margin with satellite lesions and minimal stromal vascularization. KOH mount of corneal scrapings shows branching septate hyphae. Which single feature best distinguishes this fungal ulcer from a bacterial corneal ulcer?
A. Presence of hypopyon and anterior chamber reaction
B. Ciliary injection and photophobia
C. Purulent exudate at the ulcer base
D. Slow progression with minimal stromal vascularization despite significant stromal infiltration
Explanation
Distinguishing Fungal from Bacterial Corneal Ulcers
Key Discriminating Feature
Key Point
The hallmark of fungal corneal ulcers is disproportionate stromal infiltration with minimal neovascularization — the cornea shows extensive opacity and infiltration despite relatively poor inflammatory response and minimal vessel ingrowth.
Comparative Table: Bacterial vs Fungal Corneal Ulcers
Table
Feature
Bacterial
Fungal
Speed of progression
Rapid (24–72 hrs)
Slow (days to weeks)
Stromal vascularization
Prominent, rapid
Minimal despite extensive infiltration
Margin characteristics
Sharp, undermined
Raised, indurated, feathery
Satellite lesions
Absent
Present (pathognomonic)
Hypopyon
Common, copious
Rare or minimal
Exudate
Purulent, creamy
Dry, granular
Depth of ulcer
Superficial initially
Can be deep
Pain severity
Severe
Moderate (less than bacterial)
Clinical Pearl
Clinical Pearl
Fungal ulcers are often described as having a "quiet eye" with an angry cornea" — the systemic inflammatory response (hypopyon, injection, discharge) is disproportionately mild compared to the extent of corneal destruction. This is because fungal pathogens (Aspergillus, Fusarium, Candida) trigger a delayed hypersensitivity response rather than acute suppuration.
Why This Matters in Diagnosis
High-YieldNEET PG
A patient with a corneal ulcer showing:
Extensive stromal infiltration and opacification
Minimal or absent hypopyon
Slow, indolent course
Satellite lesions
Poor response to antibiotics
...should immediately raise suspicion for fungal infection, and KOH mount / culture on Sabouraud dextrose agar should be obtained urgently.
Pathophysiology
Fungal ulcers progress slowly because:
1.
Fungal cell wall (chitin, β-glucans) does not trigger as robust a neutrophilic response as bacterial lipopolysaccharide (LPS)
2.
Fungal toxins and enzymes (keratinolytic proteases) cause direct tissue destruction rather than immune-mediated necrosis
3.
Minimal neovascularization occurs because fungal antigens do not stimulate VEGF production as effectively as bacterial endotoxins
Khurana Ophthalmology Ch 3
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.