## Crohn's Disease with Intra-abdominal Abscess **Key Point:** Management of Crohn's disease with abscess depends on abscess size, patient stability, and response to medical therapy. Percutaneous drainage (PCD) + medical management is preferred over immediate surgery when feasible. **Correct Answer: Percutaneous Drainage + Medical Management** ### Rationale: - **Abscess size (3 cm):** Suitable for percutaneous drainage (most abscesses >2 cm require drainage) - **Percutaneous drainage advantages:** - Converts emergency surgery to elective procedure - Allows time for medical optimization and immunosuppression - Reduces operative mortality and morbidity - Preserves bowel length (important in Crohn's disease) - Success rate >80% with adjunctive medical therapy - **Timing of surgery:** Elective resection 6–12 weeks after PCD and medical optimization - **Current evidence (SCCM, ASGE guidelines):** PCD + medical therapy is standard for Crohn's abscesses - **Medical therapy:** Antibiotics, mesalamine, immunosuppressants (azathioprine/biologics) ### High-Yield Mnemonic: **DRAIN** - **D**rainage for abscess >2 cm - **R**esection deferred (elective, not emergent) - **A**ntibiotics + immunosuppression - **I**mprovement with medical therapy - **N**o emergency surgery unless perforation/peritonitis ### Clinical Pearl: Emergent surgery in Crohn's disease is reserved for perforation, uncontrolled sepsis, or failed PCD. Elective surgery after medical optimization has better outcomes. 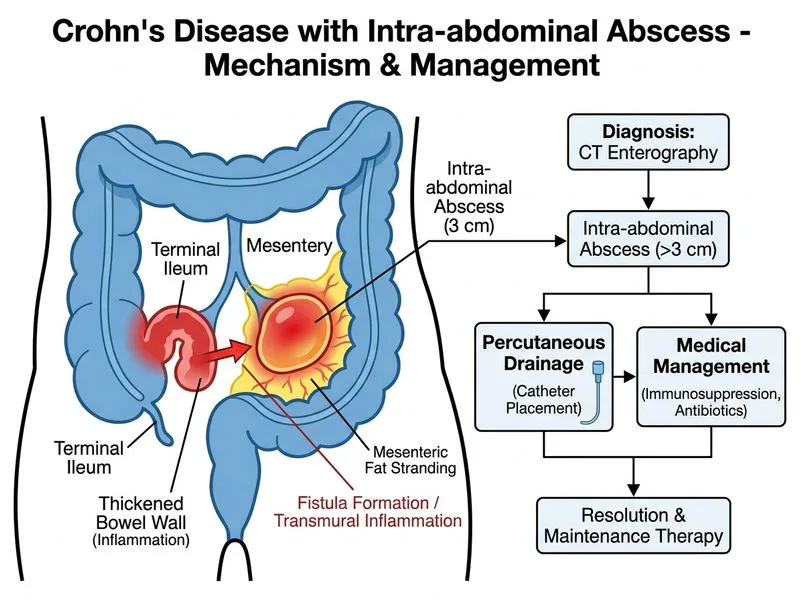
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.