A 32-year-old woman presents with a 6-week history of pruritic, scaly patches on both groins and inner thighs. Examination reveals well-demarcated erythematous plaques with a raised, advancing border and central clearing. KOH mount of scale shows branching septate hyphae. She has already used topical antifungals (clotrimazole) for 3 weeks without improvement. What is the most appropriate next step in management?
A. Continue topical clotrimazole for another 4 weeks
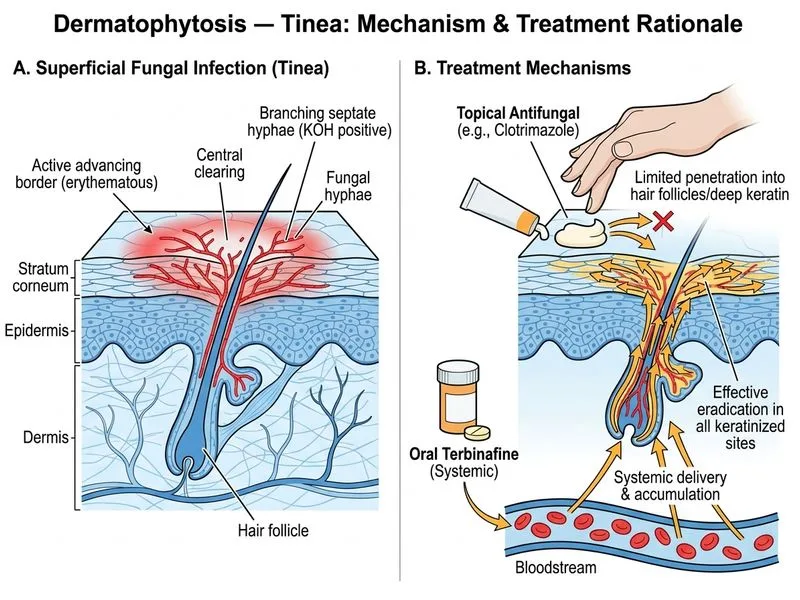
B. Start oral terbinafine 250 mg daily for 2–4 weeks
C. Perform fungal culture and await results before further treatment
D. Switch to topical miconazole and add oral fluconazole
Explanation
Clinical Context
This patient has tinea cruris (jock itch) confirmed by:
Clinical morphology: well-demarcated erythematous plaques with raised border and central clearing