A 38-year-old woman with acute promyelocytic leukemia (APL) presents to the emergency department with severe bleeding. She has epistaxis, gum bleeding, and petechiae over her trunk. Laboratory investigations reveal: Hb 7.2 g/dL, platelet count 15,000/µL, PT 18 s (control 12 s), aPTT 45 s (control 28 s), fibrinogen 85 mg/dL (normal 200–400), D-dimer markedly elevated at 8.5 µg/mL (normal <0.5). Peripheral blood smear shows abnormal promyelocytes with Auer rods. What is the most likely diagnosis?
A. Thrombotic thrombocytopenic purpura with coagulopathy
B. Immune thrombocytopenia with secondary fibrinolysis
C. Disseminated intravascular coagulation secondary to acute promyelocytic leukemia
D. Vitamin K deficiency with bone marrow suppression
Explanation
Clinical Presentation and Diagnosis
Key Point
DIC in APL is a medical emergency characterized by simultaneous activation of coagulation and fibrinolysis, leading to consumption of platelets, fibrinogen, and clotting factors.
Why This Patient Has DIC
This patient exhibits the classic pentad of DIC:
Table
Finding
Value
Significance
Thrombocytopenia
15,000/µL
Platelet consumption
Prolonged PT/aPTT
18 s / 45 s
Factor consumption
Hypofibrinogenemia
85 mg/dL
Fibrinogen consumption + fibrinolysis
Elevated D-dimer
8.5 µg/mL
Fibrin formation and degradation
Clinical bleeding
Epistaxis, petechiae
Microthrombi + factor depletion
High-YieldNEET PG
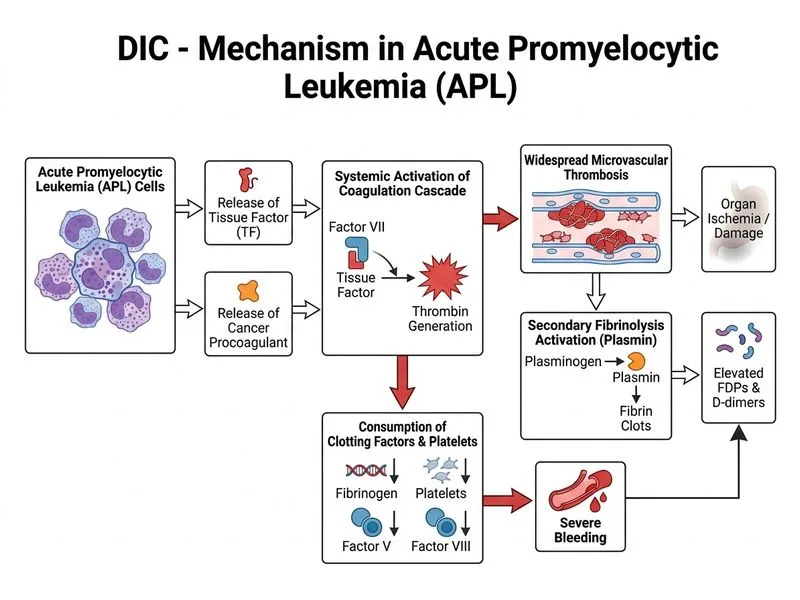
APL (t(15;17), PML-RARA fusion) is the most common malignancy associated with DIC at presentation. The leukemic promyelocytes release tissue factor (TF) and cancer procoagulant, triggering the extrinsic pathway.
Pathophysiology of DIC in APL
Loading diagram...
Clinical Pearl
The combination of prolonged PT/aPTT + thrombocytopenia + hypofibrinogenemia + elevated D-dimer in a patient with APL is pathognomonic for DIC. The Auer rods on smear confirm the APL diagnosis.
ISTH Scoring for DIC
This patient meets criteria for overt DIC:
Platelet count <100,000: 1 point
D-dimer/FDP elevation (markedly): 3 points
PT prolongation: 1 point
Fibrinogen <100 mg/dL: 1 point
Total ≥5 points = compatible with overt DIC
Mnemonic
COAGULATION — Consumption Of All clotting factors, Organ dysfunction, Activation of coagulation, Granulocytes (leukemia), Urokinase/plasmin (fibrinolysis), Low platelets, Abnormal PT/aPTT, Tissue factor release, Increased D-dimer, Organ bleeding, Necrosis of tissues.
Management Priority
1.
Immediate: Fresh frozen plasma (FFP) + cryoprecipitate for factor/fibrinogen replacement
2.
Concurrent: ATRA (all-trans retinoic acid) + chemotherapy to treat the underlying APL
3.
Avoid: Heparin is controversial in APL-DIC (risk of hemorrhage > benefit)
4.
Monitor: Serial PT, aPTT, fibrinogen, platelet count, D-dimer q6–12h
Warning
Do NOT give platelet transfusions prophylactically in DIC — they may fuel thrombosis. Transfuse only if active bleeding and platelets <10,000/µL or <20,000/µL with fever/infection.
Robbins 10e Ch 13
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.