A 52-year-old man with metastatic pancreatic adenocarcinoma presents with acute dyspnea, chest pain, and hemoptysis. On examination, he is hypotensive (BP 88/54), tachycardic (HR 118), and has cyanosis. Chest X-ray shows bilateral pulmonary infiltrates. Laboratory findings: Hb 8.5 g/dL with schistocytes on smear, platelet count 32,000/µL, PT 22 s (control 12 s), aPTT 52 s (control 28 s), fibrinogen 110 mg/dL, D-dimer 12 µg/mL. Arterial blood gas shows PaO₂ 58 mmHg on room air. What is the primary mechanism of organ dysfunction in this patient?
A. Fibrin deposition in pulmonary microvasculature leading to acute respiratory distress and microangiopathic hemolysis
B. Sepsis-induced endotoxemia with capillary leak syndrome
C. Acute left ventricular failure secondary to myocardial infarction
D. Direct tumor invasion of the pulmonary vasculature with mechanical obstruction
Explanation
DIC-Induced Multi-Organ Failure in Metastatic Cancer
Clinical Recognition of DIC with Organ Involvement
Key Point
This patient has overt DIC with acute respiratory distress syndrome (ARDS) secondary to metastatic pancreatic cancer. The primary pathophysiology is microthrombi formation in the pulmonary circulation, not mechanical obstruction or cardiac failure.
Laboratory Evidence of DIC
Table
Parameter
Finding
Interpretation
Platelets
32,000/µL
Consumption
PT/aPTT
22 s / 52 s
Factor consumption
Fibrinogen
110 mg/dL
Consumption + fibrinolysis
D-dimer
12 µg/mL
Fibrin formation & degradation
Schistocytes
Present
Mechanical hemolysis from fibrin strands
PaO₂
58 mmHg
Pulmonary dysfunction
High-YieldNEET PG
Pancreatic cancer is one of the top 3 solid tumors causing DIC (along with lung and gastric cancers). Cancer cells express tissue factor (TF) on their surface, directly activating the extrinsic coagulation pathway.
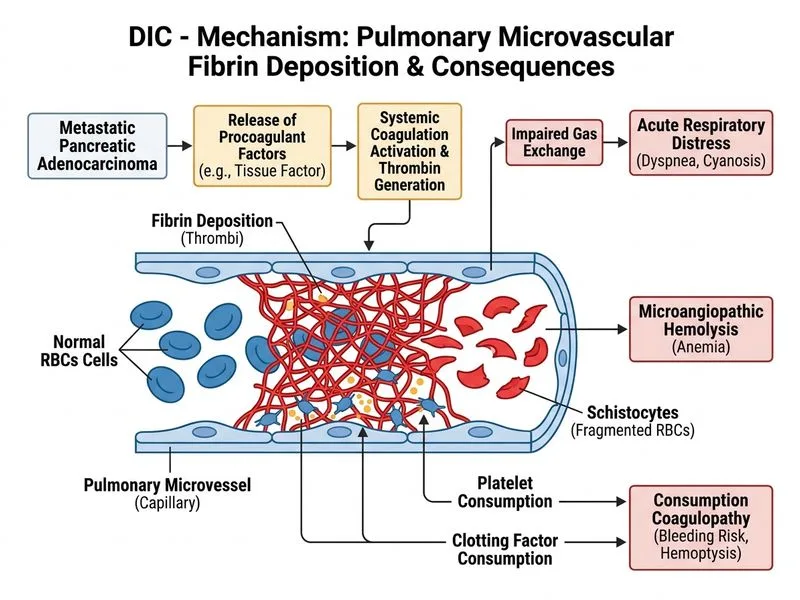
Mechanism of Pulmonary Involvement in DIC
Loading diagram...
Clinical Pearl
The combination of schistocytes + thrombocytopenia + respiratory failure + coagulopathy in a cancer patient is DIC until proven otherwise. The hemolysis is mechanical (RBCs passing through fibrin-lined capillaries), not immune-mediated.
Why This Is DIC, Not Other Diagnoses
Mnemonic
CANCER-DIC — Consumption of platelets, Abnormal PT/aPTT, Necrosis of tissues (microthrombi), Coagulation activation, Elevated D-dimer, Respiratory distress, Disseminated fibrin deposition, Ischemia of organs, Consumption of fibrinogen.
Pathophysiology of Pulmonary ARDS in DIC
1.
Microthrombi formation in pulmonary capillaries → mechanical obstruction of blood flow
2.
Endothelial injury from thrombin and fibrin deposition → increased vascular permeability
3.
Platelet and leukocyte sequestration in lungs → inflammatory cytokine release (IL-6, TNF-α, IL-8)
4.
Surfactant dysfunction from inflammatory mediators → alveolar collapse
5.
Result: Severe hypoxemia (PaO₂ 58 mmHg), bilateral infiltrates, and shock
Warning
Do NOT confuse DIC-induced ARDS with sepsis-induced ARDS. In sepsis, fibrinogen is typically elevated (acute phase reactant), whereas in DIC it is consumed and low. This patient's fibrinogen of 110 mg/dL confirms consumption, not inflammation alone.
Management Priorities
1.
Treat the underlying cancer: Chemotherapy (gemcitabine-based regimen for pancreatic cancer)
Anticoagulation: Low-dose unfractionated heparin (controversial but may reduce microthrombi formation) — use cautiously given active bleeding risk
5.
Avoid: Platelet transfusions unless active bleeding and platelets <10,000/µL
High-YieldNEET PG
The prognosis of DIC in solid tumors is poor; mortality is 40–80% despite treatment. Early recognition and aggressive management of the underlying malignancy offer the only chance of DIC reversal.
Robbins 10e Ch 13; Harrison 21e Ch 180
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.