| Investigation | Specificity for DIC | What It Measures |
|---|---|---|
| D-dimer | Highest | Cross-linked fibrin degradation; reflects both thrombin & plasmin activity |
| FDP | High but less specific | Fibrin AND fibrinogen degradation products (less specific — also elevated with fibrinogenolysis alone) |
| Platelet count | Low | Consumption (non-specific; many causes) |
| PT/aPTT | Low | Coagulation factor consumption (non-specific) |
| Fibrinogen | Low | Consumption (non-specific) |
Per the ISTH scoring system for overt DIC, D-dimer/FDP elevation is a key criterion, but D-dimer is the preferred marker in modern practice due to its superior specificity for cross-linked fibrin breakdown.
The International Society on Thrombosis and Haemostasis (ISTH) uses a composite score incorporating:
Mnemonic: STOP-DIC — Sepsis, Trauma, Obstetric complications, Pancreatitis, Disseminated malignancy (especially APL), Intravascular hemolysis, Cardiopulmonary bypass.
APL (t(15;17)) releases tissue factor and cancer procoagulants from abnormal promyelocytes, making it the highest-risk hematologic malignancy for DIC. This patient's findings (thrombocytopenia, prolonged PT/aPTT, low fibrinogen) are classic for DIC in APL.
Harrison's Principles of Internal Medicine 21e; Robbins & Cotran Pathologic Basis of Disease 10e Ch 12; ISTH DIC Scoring Guidelines
Loading illustration…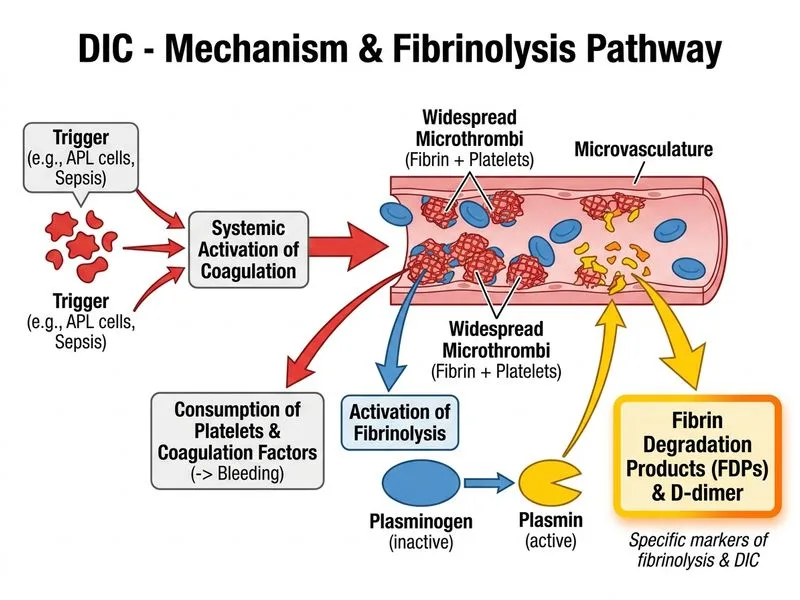
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →