A 52-year-old man with sepsis secondary to pneumonia (Gram-negative organism) presents with acute respiratory distress, hypotension, and bleeding from central line sites. Laboratory results: PT 22 sec (control 12), aPTT 52 sec (control 35), fibrinogen 110 mg/dL, platelet count 65,000/µL, D-dimer 8.5 µg/mL (normal <0.5), and schistocytes on blood smear. Blood cultures are positive. What is the most appropriate immediate next step in management?
A. Start fresh frozen plasma and cryoprecipitate, then begin warfarin for long-term anticoagulation
B. Administer broad-spectrum antibiotics, fluid resuscitation, vasopressors, and supportive transfusion of FFP/platelets/RBCs as needed
C. Initiate therapeutic anticoagulation with unfractionated heparin to prevent microvascular thrombosis
D. Perform plasmapheresis immediately to remove circulating tissue factor and DIC mediators
Explanation
Clinical Context: Sepsis-Induced DIC
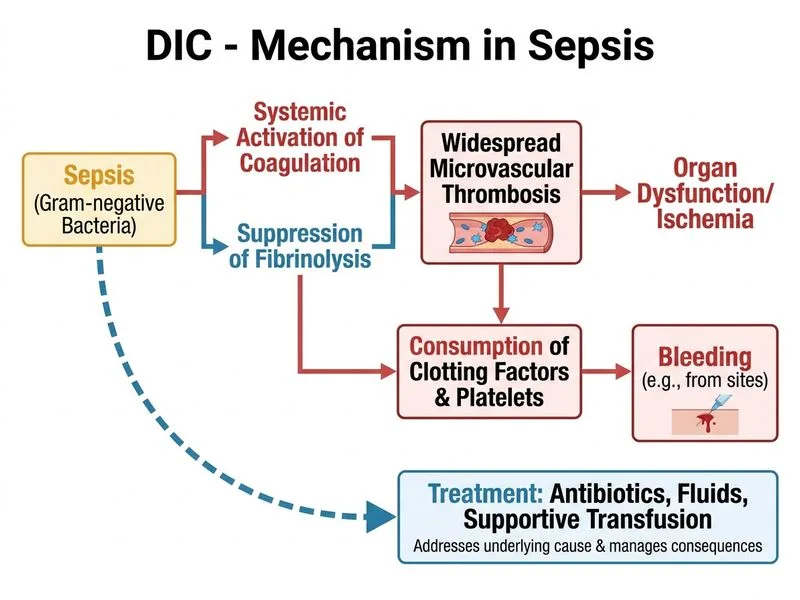
This patient has DIC secondary to septic shock, the most common cause of DIC in adult ICUs. The pathophysiology involves endotoxin-mediated activation of tissue factor (TF) on monocytes and endothelial cells.
Diagnostic Criteria Met (ISTH DIC Score)
Table
Parameter
Finding
Interpretation
Platelet count
65,000/µL
Moderate thrombocytopenia
D-dimer/FDP
8.5 µg/mL (markedly ↑)
Massive fibrin formation
PT prolongation
22 sec
Clotting factor consumption
Fibrinogen
110 mg/dL
Mild-moderate hypofibrinogenemia
Schistocytes
Present
Microangiopathic hemolytic anemia
High-YieldNEET PG
ISTH DIC score ≥5 = overt DIC. This patient scores ≥5 and requires immediate management.
Pathophysiology of Sepsis-DIC
Loading diagram...
Why This Answer Is Correct
Key Point
The cornerstone of sepsis-DIC management is treatment of the underlying infection and hemodynamic support, NOT anticoagulation.
1.
Antibiotics: Broad-spectrum coverage (e.g., piperacillin-tazobactam + fluoroquinolone or carbapenem) to control bacteremia and reduce endotoxin release.
2.
Fluid resuscitation + vasopressors: Restore perfusion pressure and prevent organ failure (SOFA score reduction).
3.
Supportive transfusion: FFP for clotting factor replacement, cryoprecipitate for fibrinogen (target >100 mg/dL in bleeding), platelets if <50,000/µL or <100,000/µL with active bleeding, RBCs for anemia.
4.
Why NOT anticoagulation: Heparin does not improve outcomes in sepsis-DIC and increases bleeding risk. DIC resolves when infection is controlled.
Clinical Pearl
Sepsis-DIC is a prothrombotic state masquerading as bleeding disorder. The primary pathology is microvascular thrombosis (schistocytes, organ failure), not consumption coagulopathy. Anticoagulation worsens bleeding without improving survival.
High-YieldNEET PG
The PROWESS trial and subsequent sepsis guidelines (Surviving Sepsis Campaign) recommend against routine anticoagulation in sepsis-DIC. Focus on source control and supportive care.
Harrison 21e Ch 325; Surviving Sepsis Campaign Guidelines 2021
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.